
 |
| Image Credit: Pixabay |
 |
| This post was peer reviewed. Click to learn more. |
Author: Patrick M. Brown, MSIV
Western University of Health Sciences College of Osteopathic Medicine of the Pacific
Case
An otherwise healthy 25 year old male is brought to the emergency department (ED) by emergency medical services (EMS) after witnesses saw him collapse while hiking in Arizona on a humid 38.3°C (101°F) summer day. His friends state that he was feeling well and behaving normally before hiking and add that they found his full water bottle in the car on the way to the ED. On physical exam, his temperature is 40.6°C (105.2°F), pulse is 134, blood pressure is 82/60, O2 saturation is 88% on room air and respirations are 21 breaths/min and labored. BMI is 29.3. He currently is unable to answer questions appropriately and appears restless. He is diaphoretic and hot to the touch. Eye exam reveals pupils that are 3mm and reactive to light bilaterally. Crackles are heard bilaterally on lung auscultation. Neurological exam reveals no abnormalities in tone or reflexes and the neck is supple. There are no obvious signs of trauma. His friends state that he is a regular smoker, social drinker and smokes marijuana recreationally. Labs significant for hemoglobin of 17.2, hematocrit of 51.0, WBC of 16.9, BUN of 43, creatinine of 0.9, and 2+ ketones in urine.
Cooling measures are initiated. Intravenous fluid boluses are running. ABG shows PaO2 of 52 mmHg. The patient is intubated and admitted to the intensive care unit.
Discussion
This adult male is suffering from exertional heat stroke (EHS) with subsequent acute respiratory failure requiring intubation. Collapsing during strenuous exercise on a hot day is typical for EHS and the diagnosis can be made based on history with core temperature > 40°C and central nervous system involvement including (but not limited to) syncope, altered mental status, and seizures.[1] Exertional heat exhaustion is on the spectrum for EHS, but presents without central nervous system dysfunction. The workup should start with an electrocardiogram to rule out cardiac causes of syncope, including cardiac arrest or arrhythmia. In a young adult athlete, hypertrophic cardiomyopathy is a good differential diagnosis for exertional syncope. Fingerstick glucose, urinalysis, complete metabolic panel, complete blood count, creatinine kinase, liver function tests, thyroid stimulating hormone, and coagulation studies should be obtained to assess etiologies and end organ damage.[2] 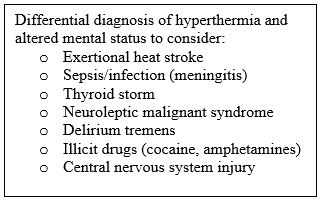
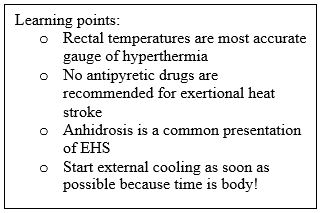
On hot days with high humidity, the body’s sweat cooling mechanism can be overwhelmed and ultimately fail to cool the body, leading to a potentially dangerous rise in core temperature. Dehydration can ensue and lead to end organ dysfunction, as evidenced by this patient’s pre renal azotemia, hemoconcentrated labs, and urine ketones. Although the vital signs and lab results meet systemic inflammatory response syndrome criteria and can mimic sepsis, the elevated white blood cell count is likely due to demarginalization and stress reaction. One of the most important teaching points of EHS is that it can both present with heavy sweating or lack of sweating (anhidrosis).[1,2,4]
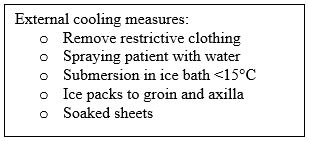 Just like in a typical stroke, where “time is brain, for EHS “time is body,” as mortality is significantly affected by how long it takes for cooling measures to be initiated.[3] Thus, ED physicians should be keenly aware of the cooling protocol at their ED and how to quickly implement it. EMS will often start rudimentary cooling procedures en route. When presented with a patient with EHS, the first line treatment is establishing intravenous (IV) access, placing the patient on a cardiac monitor, and intubation if necessary. Of note, the most accurate way of assessing core temperature is rectally, as oral temperatures are often inaccurate.[2] Urgent external cooling measures within 30 minutes and management of end organ complications are first line. Removal of clothing and ice water submersion in water under 15° C should be used to decrease the temperature by 0.2 C°/min and cease once the patient’s temperature reaches 38.3°C. Submersion in ice water will usually cool the patient in 20-40 minutes.[3] IV fluid resuscitation, possibly with D50W if the patient is hypoglycemic, should be also started immediately. Benzodiazepines should be given if the patient is having a seizure, and electrolytes should be corrected. A key point for the treatment of EHS is that antipyretic medications are not recommended.[1] In fact, there is no pharmacological treatment recommended for EHS, as NSAIDs and acetaminophen can exacerbate end organ damage!
Just like in a typical stroke, where “time is brain, for EHS “time is body,” as mortality is significantly affected by how long it takes for cooling measures to be initiated.[3] Thus, ED physicians should be keenly aware of the cooling protocol at their ED and how to quickly implement it. EMS will often start rudimentary cooling procedures en route. When presented with a patient with EHS, the first line treatment is establishing intravenous (IV) access, placing the patient on a cardiac monitor, and intubation if necessary. Of note, the most accurate way of assessing core temperature is rectally, as oral temperatures are often inaccurate.[2] Urgent external cooling measures within 30 minutes and management of end organ complications are first line. Removal of clothing and ice water submersion in water under 15° C should be used to decrease the temperature by 0.2 C°/min and cease once the patient’s temperature reaches 38.3°C. Submersion in ice water will usually cool the patient in 20-40 minutes.[3] IV fluid resuscitation, possibly with D50W if the patient is hypoglycemic, should be also started immediately. Benzodiazepines should be given if the patient is having a seizure, and electrolytes should be corrected. A key point for the treatment of EHS is that antipyretic medications are not recommended.[1] In fact, there is no pharmacological treatment recommended for EHS, as NSAIDs and acetaminophen can exacerbate end organ damage!
One of the most feared complications of EHS is acute respiratory distress syndrome (ARDS) leading to respiratory failure. Our patient has hypoxia, crackles on exam and respiratory failure on ABG which signal a developing ARDS. Other sequelae can include disseminated intravascular coagulation, seizures, renal failure, rhabdomyolysis, hepatic failure, and ultimately death.[4]
 Unfortunately, EHS cases continue to be prevalent amongst athletes, military recruits and workers and those who engage in physical activity in hot climates. Other risk factors include obesity, poor acclimatization, subpar physical fitness and preceding dehydration.[1,2] A key cohort to watch for EHS is American high school football players who often practice twice a day during hot summer months at the start of their season when their fitness might not be optimal. EHS occurs in 4.5 to every 100,000 exposed high school football players, but could be prevented by frequent breaks and adequate hydration.[5]
Unfortunately, EHS cases continue to be prevalent amongst athletes, military recruits and workers and those who engage in physical activity in hot climates. Other risk factors include obesity, poor acclimatization, subpar physical fitness and preceding dehydration.[1,2] A key cohort to watch for EHS is American high school football players who often practice twice a day during hot summer months at the start of their season when their fitness might not be optimal. EHS occurs in 4.5 to every 100,000 exposed high school football players, but could be prevented by frequent breaks and adequate hydration.[5]
For ED physicians, recognizing the signs and symptoms of EHS and treating quickly can prevent end organ damage and even death. Certainly, education is needed both for both athletes and the rest of the lay public regarding EHS to prevent this avoidable but deadly condition.
References
1. Bouchama A, Knochel JP. Heat Stroke. New England Journal of Medicine. 2002; 346(25):1978-1988.
2. Becker JA, Stewart, LK. Heat Related Illness. American Family Physician. 2011 Jun 1;83(11):1325-30.
3. Casa DJ, McDermott BP, Lee EC, Yeargin SW, Armstrong LE, Maresh CM. Cold Water Immersion: the gold standard for exertional heatstroke treatment. Exercise and Sport Sciences Reviews. 2007:141-149.
4. Leon LR, Helwig BG. Heat stroke: Role of the systemic inflammatory response. Journal of Applied Physiology. 2010;109(6):1980-1988.
5. Yard EE, Gilchrist J, Haileyesus T, et al. Heat illness among high school athletes — United States, 2005–2009. Journal of Safety Research. 2010;41(6):471-474.