
 |
| This post was peer reviewed. Click to learn more. |
Authors: Alexandria Gregory, MS-2
Saint Louis University School of Medicine
AAEM/RSA Social Media Committee
Eric Goedecke, DO
Milford Regional Medical Center
Overview
A 22-year-old female with a history of nasal polyps presented to the emergency department (ED) reporting a polyp in her nose that she noticed several days prior, as well as a growth in her throat that appeared approximately eight hours prior to evaluation. She also reported chills earlier in the week as well as a sore throat. The patient had a history of nasal polyp removal several years prior, but was not currently being followed by Otolaryngology.
On exam, there was a mass adjacent to the left lateral uvula, approximately 1.5-2 cm in length and 1 cm in width, appearing to originate from the palate. The mass was purple in color with some areas of scattered opacity. Tonsillar pillars and uvula were normal. There was a clear nasal polyp in the anterior left nare. The patient had bilateral submandibular adenopathy.
 |
|
Figure 1: Oropharyngeal exam
Image Credit: Eric Goedecke, DO |
Diagnosis
As the source of the mass was unclear, Otolaryngology was consulted, and recommended obtaining basic labs and neck soft tissue computed tomography (CT). A complete blood count and basic metabolic panel were unremarkable. Soft tissue neck CT showed a soft tissue mass filling the left maxillary sinus, extending into the left nasal cavity and oropharynx. The appearance of the mass was most consistent with an antrochoanal polyp.
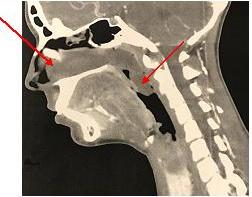 |
| Figure 2: Soft tissue neck computed tomography |
Management
Otolaryngology evaluated the patient in the ED and patient was given dexamethasone and observed. After several hours, the mass appeared largely unchanged, so the patient was admitted and scheduled for the operating room (OR), as there was the potential for airway obstruction. In the OR, the diagnosis of left antrochoanal polyp with nasopharyngeal and oropharyngeal extension was confirmed, and the polyp was removed via functional endoscopic sinus surgery (FESS). The oropharyngeal component was hemorrhagic in appearance. There were no complications, and the patient was discharged home on antibiotics and instructed to follow up with Otolaryngology as an outpatient.
Discussion
Antrochoanal polyps are benign lesions that extend from the maxillary antrum to the choana. The antral component is typically cystic, while the extension is usually solid. They are almost always unilateral, and patients typically present with nasal obstruction and nasal drainage. Antrochoanal polyps are more common in children and young adults, and more often seen in males than females.[1]
While growth of antrochoanal polyps is typically slow, and can often occur over a period of years, complications may cause acute concerns. Such complications include edema, hemorrhage, and vascular thrombosis.[2] This patient experienced hemorrhaging, which accelerated the growth of the polyp overnight. In the ED, the primary concern regarding antrochoanal polyps is airway obstruction.
The definitive treatment for antrochoanal polyps is always surgical. FESS is now the most commonly used technique, and is generally associated with a low rate of recurrence. This method preserves healthy antral mucosa and is associated with a shorter recovery time. The Caldwell-Luc approach, in which the maxillary sinus mucosa is removed, has the lowest rate of recurrence, but has more associated risks, especially in younger children.[3] The most important factor in preventing recurrence is to remove the polyp completely, as incomplete removal has a 25% recurrence rate. Otherwise, patients are typically cured following complete surgical excision.[2]
References:
1. Yaman H, Yilmaz S, Karali E, Guclu E, Ozturk O. Evaluation and management of antrochoanal polyps. Clin Exp Otorhinolar. 2010;3(2):110-114. doi:10.3342/ceo.2010.3.2.110.
2. Wenig, B. Atlas of head and neck pathology. 2nd ed. Philadelphia, PA: Saunders; 2007.
3. Saafan M, Tomoum M. Study of recurrent antrochoanal polyps: causes and how to minimize recurrence. Egypt J Otolaryngol. 2012;28:75-79.