
 |
| Image Credit: Dr. Wanner |
 |
| This post was peer reviewed. Click to learn more. |
Authors: Gregory Wanner, DO
Emergency Physician/Clinical Faculty
Christiana Care Health System
@gregwanner
Paul Kolecki, MD
Associate Professor, Emergency Medicine
Medical Toxicologist
Thomas Jefferson University
An 18-year-old male presents to the emergency department (ED) stating, “Doc, I’m really drunk.” He and a friend were drinking in the friend’s garage. The patient drank one “very strong” sweet-smelling drink, which was prepared by his friend. He began to feel sick and nauseated and rode his bike home (with difficulty due to this intoxication, but without any falls or trauma). He vomited twice and his mother referred him to the ED. Attempts to contact the friend were unsuccessful.
How would you evaluate this patient?
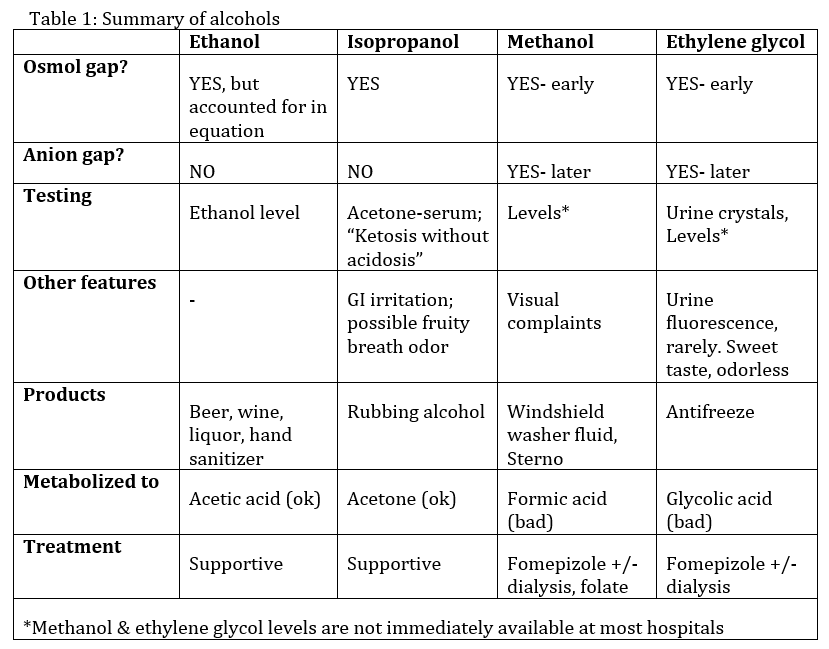
Several intoxicants can cause similar symptoms. While ethanol is the most likely cause, in patients with unclear ingestions other alcohols should be considered as well. The following is a brief summary of the alcohols often tested on in-service and board exams; a summary table is included at the end:
The “alcohols” we will discuss:
- Ethanol
- Isopropanol
- Methanol
- Ethylene glycol
Signs and Symptoms:
Each of these alcohols can cause similar intoxication symptoms. We are quite familiar with the symptoms of ethanol intoxication; however, the other alcohols have some additional defining features which are easily testable on an in-service or board exam: [1,5-7]
- Isopropanol: GI irritation and is 2-3 times more potent than ethanol, per volume
- Methanol: Visual complaints
- Ethylene glycol: Renal failure, sometimes seizures
Workup:
Obtaining an appropriate history is most important. Start by asking the patient about alcohol or drug use and the types of alcohol or drugs used. Asking about suicidal thoughts is also important. Cases of clear-cut ethanol ingestion, confirmed by a reliable patient or family/friend, typically do not require an evaluation for toxic alcohols. Patients with suicidal ideations and an unclear ingestion, unknown types of alcohol-like ingestions (such as our example above), or patients admitting to ethylene glycol/methanol use should raise concerns. In cases concerning for toxic alcohol ingestion, the initial workup should include a finger-stick glucose, basic metabolic panel, ethanol level, urinalysis, serum osmolality, and venous blood gas. Methanol and ethylene glycol levels are “send out” tests at most facilities, limiting the clinical utility of these tests in the ED. However, if methanol or ethylene glycol ingestion is suspected, these levels should be sent and followed by the admitting team. Additional testing, such as acetaminophen and salicylate levels, and an EKG should also be considered in cases of uncertain ingestions. It is also important to calculate the anion gap and osmol gap.[1,3,5-7]
- · Osmol gap:
- All alcohols discussed will have an elevated osmol gap shortly after ingestion (remember to include ethanol in the osmolality calculation).
- Osmol gap >50 is highly suggestive of toxic alcohol poisoning (especially methanol or ethylene glycol), but the osmol gap doesn’t have to be this high.[3]
- To calculate osmol gap:
- Go to MDCalc,[8] or get out your calculator and do the following two calculations:
- Serum osmolality = (Na x 2) + (glucose/18) + (BUN/2.8) + (ethanol/3.7)
- Osmol gap= measured serum osmolality – calculated serum osmolality
- Normal ranges -14 to +10 (per Goldfrank’s toxicology) [3]
- Anion gap:
- Ethanol and isopropanol—NO elevated anion gap
- Ethylene glycol and methanol—YES elevated anion gap BUT begins to elevate as the toxic alcohols are metabolized.
- The anion gap goes up as osmol gap goes down
- Elevation of the anion gap takes time: ethylene glycol usually within 6 hours, methanol can take 16 hours or more.
- Side note: Propylene glycol
- An ingredient in environmentally “safe” antifreeze and a diluent for many medications (such as lorazepam or phenytoin)
- Toxicity can occur when medications (such as phenytoin) containing propylene glycol are infused too rapidly.
- Can cause an elevated anion gap (ICU patient on lorazepam drip)…otherwise, don’t worry about it.
- ·Ketones:
- Check urine ketones and consider ordering an acetone level (if available).
- “Ketosis without acidosis” is diagnostic of isopropanol ingestion/intoxication.[1-3]
Treatment:
Ethanol or Isopropanol: [1,2,5]
- Monitor, supportive care, and “metabolize to freedom”
Methanol or Ethylene Glycol: [3,4,6,7]
- Call poison control: 800-222-1222
- Metabolic blockade (Fomepizole or Ethanol)
- Blocks alcohol dehydrogenase
- Indications:
- Documented methanol/ethylene glycol level >20mg/dL
- Concern for significant ingestion, no level immediately available, AND
- Unexplained serum osmolar gap >10 mOsm/L, OR
- Unexplained metabolic acidosis and ETOH less than 100.
- Fomepizole:
- Loading dose 15mg/kg IV over 30 minutes, then 10mg/kg q12h for 4 doses, then 15mg/kg q12h until the ethylene glycol/methanol level is <20 mg/dL.
- Ethanol: (good trivia, but rarely used)
- IV dosing: 10mL/kg of 10% IV solution) then ~1.2 mL/kg/h of 10% IV solution
- PO dosing: 3-4 1oz shots of 80 proof liquor, then 1-2 shots/hr
- Keep the ethanol level between 100-150 mg/dL
- Check the blood glucose frequently
- Metabolic blockade is continued until methanol/ethylene glycol level is <20 and metabolic acidosis resolves.
- Hemodialysis Indications:
- Refractory metabolic acidosis (pH<7.25 w/ AG >30 and/or base deficit <-15).
- Visual abnormalities (methanol) or renal insufficiency (ethylene glycol).
- Deteriorating vitals or worsening electrolyte abnormality.
- Serum methanol or ethylene glycol level >50mg/dL (relative indication).
- Disposition Planning:
- Symptoms can be delayed (especially if ethanol is a co-ingestant)
- Admit and refer the admitting team to poison control for ongoing management
Conclusion:
Intoxicated patients frequently end up in the ED. Emergency physicians should consider the possibility of toxic alcohol ingestion, both clinically and while answering board-style test questions.
References:
1. Slaughter RJ, Mason RW, Beasley DM, Vale JA, Schep LJ. Isopropanol poisoning. Clin Toxicol (Phila). 2014;52(5):470-8. PMID: 24815348
2. Stremski E, Hennes H. Accidental isopropanol ingestion in children. Pediatr Emerg Care. 2000;16(4):238-40. PMID: 10966340
3. Wiener SW. Toxic Alcohols. In: Nelson LS, Lewin NA, Howland MA, Hoffman RS, Goldfrank LR, Flomenbaum NE, eds. Goldfrank’s Toxicologic Emergencies 10th ed. NewYork: McGraw Hill Medical; 2015:1346-1347.
4. Buchanan JA, Alhelail M, Cetaruk EW, et al. Massive ethylene glycol ingestion treated with fomepizole alone-a viable therapeutic option. J Med Toxicol. 2010;6(2):131-4. PMID: 20422336
5. Watts DJ, Bendas C. Isopropyl Alcohol. In: Kazzi ZN, Shih R, eds. AAEM Resident & Student Association Toxicology Handbook, 2nd ed. AAEM/RSA; 2011.
6. Watts DJ, Horrell D. Ethylene Glycol. In: Kazzi ZN, Shih R, eds. AAEM Resident & Student Association Toxicology Handbook, 2nd ed. AAEM/RSA; 2011.
7. Watts DJ, Fumanti BJ. Methanol. In: Kazzi ZN, Shih R, eds. AAEM Resident & Student Association Toxicology Handbook, 2nd ed. AAEM/RSA; 2011.
8. Serum Osmolality/Osmolarity. MDCALC. Available at: http://www.mdcalc.com/serum-osmolality-osmolarity/. Accessed October 28, 2016.