
 |
| Image Credit: Flickr Andrew Ranta |
Author: Kaylinn Dokken, OMSIV
Western University of Health Sciences
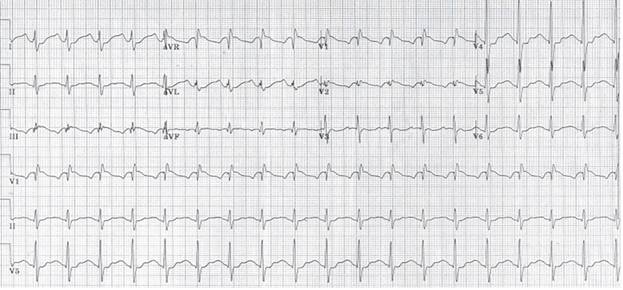
You are just at the beginning of your shift when paramedics call in and notify you that they are bringing in a 35 year old female who reports that she took 3,000 mg of diphenhydramine in a suicide attempt. Her BP is 145/80, her pulse is 160 beats per minute (bpm) with sinus tachycardia on the monitor, and her respiratory rate is 24 breaths per minute. Upon presentation, the patient is disoriented, continuously writhing, and having intermittent myoclonic jerks. An initial EKG is obtained and is shown below.
 |
| EKG #1, used with permission [1] |
Background
Diphenhydramine (sometimes abbreviated as “DPHM”) is a 1st generation H1 blocker, commonly associated with sedation. Presenting symptoms of an overdose depend on the amount taken and the overall metabolism of the drug by the patient. The symptoms are due the blockade of sodium channels, leading to dysfunction of the cardiac and central nervous systems.[2] Diphenhydramine overdoses can present with anticholinergic effects such as mucosal dryness, elevated temperature, urinary retention, mydriasis (leading to blurred vision), altered mental status, hypertension, and tachycardia.[3] In addition the drug can affect the smooth muscle of the GI tract and the urinary bladder, leading to ileus and urinary retention.
Cardiac Effects
One of the most common symptoms in diphenhydramine overdose is tachycardia. The majority of patients will have heart rates greater than 90bpm, with a smaller number of patients having heart rates greater than 120 bpm.[4]
At low doses diphenhydramine works by inhibiting the fast sodium channels, and at higher doses it inhibits potassium channels leading to QT prolongation.[5] In addition to QT prolongation, there have been numerous instances of QRS widening to >100ms due to a prolonged phase 0 depolarization.[6]
 |
| Image from Wikimedia; original author Quasar, derivative work by Mnokel and Silvia3: https://commons.wikimedia.org/wiki/File:Action_potential_ventr_myocyte.gif |
{kind=link}
In one analysis of patients with diphenhydramine overdoses, more than half of the patients had QTc intervals >450ms with a smaller percentage having more significant prolongation.[4] In some cases QTc prolongation leads to the development of torsades de pointes. If this occurs, the patient should be treated with 1-2 g of IV magnesium sulfate over 1-2 minutes, or defibrillation if the patient is pulseless.[7] In a patient who has pulses and is unresponsive to magnesium, overdrive pacing can be considered (initiating the pacing rate at 90-100 and gradually increasing until termination of torsades).
Tachycardia in diphenhydramine overdose can be either wide or narrow complex, and often mimics a tricyclic antidepressant overdose. Therefore, it is very important to have the patient on continuous ECG monitoring to observe for excessive widening of the QRS interval or QTc prolongation. If you start to witness QRS widening (>100 ms), treat with 1-2mEq/kg of sodium bicarbonate.[6-8] The narrowing of the QRS complexes should be seen within 30-60 seconds of administration of the bicarbonate. If the initial dose of bicarbonate does not lead to narrowing of the QRS, additional doses of sodium bicarbonate can be given.[7] There have been some case reports of patients receiving over 500mEq of bicarbonate before seeing narrowing.[2] If QRS widening persists, then you should consider initiating a continuous infusion of sodium bicarbonate and a rate of 2-5mEq/kg over 4-8 hours, titrating to effect.[7] Sodium bicarbonate works by increasing the sodium gradient in the channels.[6]
 |
| EKG #2, after sodium bicarbonate, used with permission[1] |
Central Nervous System Effects
Changes in mental status often accompany diphenhydramine overdose. Most commonly, patients have disorientation and unconsciousness; these symptoms are present in over 40% of patients with overdose.[4] Patients can also present with seizures or psychosis, which are more common with severe overdoses.[9] The treatment of choice in these cases is medical management focused on controlling symptoms, and includes using medications such as benzodiazepines.
Disposition
Now that we know how diphenhydramine overdose can present, what do we do about the disposition of the patient? While severe overdoses, like the one presented here, will require ICU level care, knowing the total ingested dose can be a guide to estimate the likelihood of clinical deterioration. According to one study, there is a critical dose limit for diphenhydramine that represents high risk for rapid deterioration of a patient’s condition. Patients who have taken 1 gram or greater require hospitalization. These patients are at grave risk for developing severe symptoms, which include delirium, psychosis, seizures, and coma.[9] These patients will require a higher level of care and monitoring based on their risk of deterioration.
As a side note, this critical dose limit applies to patients without any comorbidities. In patients with comorbid conditions or ingestion of additional substances, these severe symptoms can be seen at much lower doses.[9]
Summary
Diphenhydramine is widely available and has the potential to be used in suicide attempts. While the doses required to cause substantial harm are quite high, the potential adverse effects on the cardiovascular and central nervous system are common, potentially fatal, and must be monitored closely. Patients who have taken over 1 gram of diphenhydramine are at increased risk of severe reactions and must be admitted for further monitoring.
References
1. Jang D, Manini A, Trueger N et al. Status epilepticus and wide-complex tachycardia secondary to diphenhydramine overdose. Clinical Toxicology. 2010;48(9):945-948. doi:10.3109/15563650.2010.527850. PMID: 21171853
2. Abdi A, Rose E, Levine M. Diphenhydramine Overdose with Intraventricular Conduction Delay Treated with Hypertonic Sodium Bicarbonate and IV Lipid Emulsion. WestJEM. 2014;15(7):855-858. doi:10.5811/westjem.2014.8.23407. PMID: 25493135
3. Emadian S, Caravati E, Herr R. Rhabdomyolysis: A rare adverse effect of diphenhydramine overdose. The American Journal of Emergency Medicine. 1996;14(6):574-576. doi:10.1016/s0735-6757(96)90103-5. PMID: 8857809
4. Zareba W, Moss A, Rosero S, Hajj-Ali R, Konecki J, Andrews M. Electrocardiographic Findings in Patients With Diphenhydramine Overdose. The American Journal of Cardiology. 1997;80(9):1168-1173. doi:10.1016/s0002-9149(97)00634-6. PMID: 9359544
5. Sype J, Khan I. Prolonged QT interval with markedly abnormal ventricular repolarization in diphenhydramine overdose. International Journal of Cardiology. 2005;99(2):333-335. doi:10.1016/j.ijcard.2003.11.035. PMID: 15749198
6. Sharma A, Hexdall A, Chang E, Nelson L, Hoffman R. Diphenhydramine-induced wide complex dysrhythmia responds to treatment with sodium bicarbonate. The American Journal of Emergency Medicine. 2003;21(3):212-215. doi:10.1016/s0735-6757(02)42248-6. PMID: 12811715
7. Greenwood J. PressorDex 2nd Ed. Irving, TX: Emergency Medicine Residents Association; 2015.
8. Smollin C. Call Us!…The Official Newsletter of the California Poison Control System. 2007;5(1). Available at: http://www.calpoison.org/hcp/2007/callusvol5no1.htm. Accessed May 10, 2015.
9. Radovanovic D, Meier P, Guirguis M, Lorent J, Kupferschmidt H. Dose-dependent toxicity of diphenhydramine overdose. Human & Experimental Toxicology. 2000;19(9):489-495. doi:10.1191/096032700671040438. PMID: 11204550