
 |
| This post was peer reviewed. Click to learn more. |
Author: Daniel Balk, MD
Emergency Medicine Resident
Drexel University College of Medicine
The Case:
The tech hands the physician this EKG:
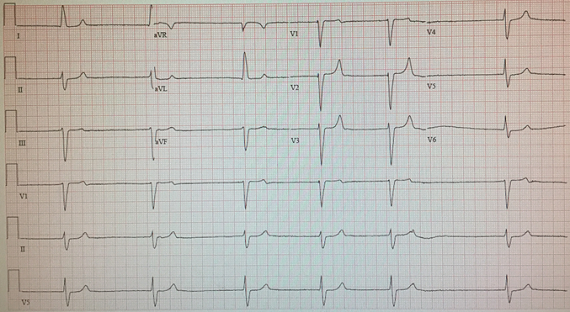
It’s slow with a rate of 37, it’s irregular, it’s wide with a QRS of 130, it’s scary, and there is no previous EKG. The tech doesn’t know the patient’s story as “he speaks only Portuguese” and his chief complaint is hypoglycemia.
Glancing at the monitor as the physician rushes towards the room, the blood pressure is 138/71. This elderly Brazilian traveller (with a prior history of two cardiac stents, hypertension and diabetes) is discussing with his family whether his two days of diarrhea caused his sugar to be low all day despite foregoing his insulin. His blood glucose was 40 this morning; it’s 135 now after eating normally all day and skipping his long acting and mealtime insulin doses. The review of systems is entirely negative other than for diarrhea and hypoglycemia. Other than marked bradycardia, the exam is unremarkable.
What’s going on? He looks stable despite having this EKG. The physician orders placement of pacer pads and 0.5mg of atropine, giving a few moments to think.
So, what’s on the differential?[1]
- Ischemia, particularly RCA
- Heart block
- Hypoxia
- Toxicological: calcium channel blocker, beta blocker, digoxin, organophosphates
- Sick sinus syndrome
- Neurogenic: increased ICP, vasovagal
- Metabolic/endocrine: hypothyroid, hyperkalemia, hypothermia
- Infectious: Chagas disease, Lyme disease
The Case Continued
Could this be hyperkalemia from renal failure? This would explain the hypoglycemia. Acute renal failure can impair insulin clearance causing his blood sugar to drop; and a marked hyperkalemia can also produce a very lethal bradycardia.
The critical care panel comes back quickly with a potassium of 8.0. His creatinine later returns at 7.0. The physician immediately temporizes him with calcium gluconate, sodium bicarbonate, insulin and D50. Just minutes after getting his first amp of calcium gluconate his QRS starts to narrow; the repeat EKG looks like this:
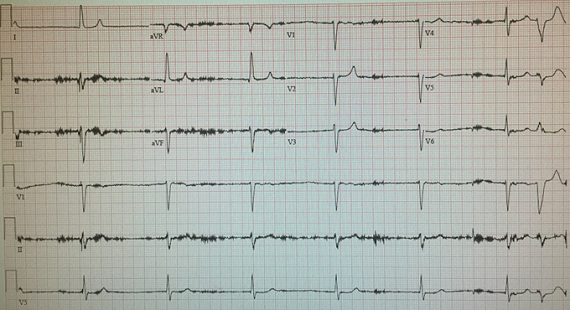
When we suspect hyperkalemia, we’ve all had the EKG progression ingrained. First, there are peaked T waves with or without QT shortening. Next comes PR lengthening and QRS widening, with possible loss of the P wave. This, of course, can progress to the dreaded sine wave.
What other EKG changes can hyperkalemia cause? It turns out that hyperkalemia can do just about anything to the EKG. It can affect all of the intervals: PR, QRS, or QT. It can lead to conduction delays including LBBB, RBBB, and fascicular blocks.[2] It can cause arrhythmias such as sinus bradycardia, ventricular tachycardia, ventricular fibrillation, idioventricular rhythms, and asystole.[3,4] It can cause loss of P waves or even a Brugada pattern.[5] In this particular case, the patient developed an irregular bradycardic idioventricular rhythm with QRS widening. With just about any abnormal EKG, hyperkalemia has to be on the differential.
The Case Resolved
The patient went to the critical care unit, where his hyperkalemia began to resolve with aggressive fluid resuscitation. The next morning his potassium was down to 5.2; his EKG is shown below:
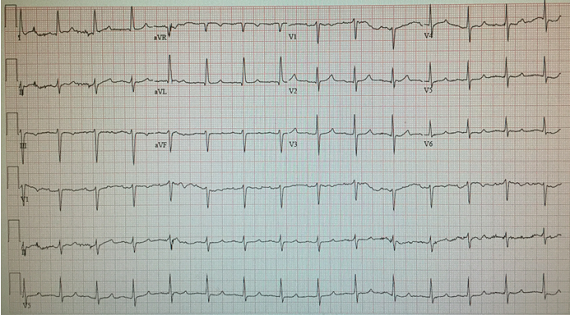
We must carry a high index of suspicion for this diagnosis. Otherwise, we may miss a highly lethal, but highly treatable cause of bradycardia.
References:
- Mottram AR, Svenson JE. Rhythm Disturbances. Emergency Medicine Clinics of North America. 2011;29(4):729-746
- Bashour T, Hsu I, Gorfinkel HJ, et al. Atrioventricular and Intraventricular Conduction in Hyperkalemia. American Journal of Cardiology. 1975;35:199
- Greenberg A. Hyperkalemia: Treatment Options. Seminars in Nephrology. 1998;18:46
- Mattu A, Brady WJ, Robinson DA. Electrocardiographic Manifestations of Hyperkalemia. American Journal Emergency Medicine. 2000;18:721
- Littmann L, Monroe MJ, Taylor L, Brearley WD. The Hyperkalemic Brugada Sign. Journal of Electrocardiology. 2007;40:53