
 |
| This post was peer reviewed. Click to learn more. |
Authors: Benjamin Lindquist, MD
Emergency Medicine Chief Resident
Stanford/Kaiser Emergency Medicine Residency
Cameron McClure, MD FACEP
Emergency Physician
The Permanente Medical Group, Santa Clara, CA
Jamie Chang, MD MBA
Emergency Physician
The Permanente Medical Group, Santa Clara, CA
A 21-day-old previously healthy male was brought to the emergency department by his parents approximately one hour after he developed right-sided scrotal swelling. According to his parents, he was noted to be less active during the day. They denied fevers or vomiting and reported that he was making adequate urine. He was also having normal, non-bloody bowel movements.
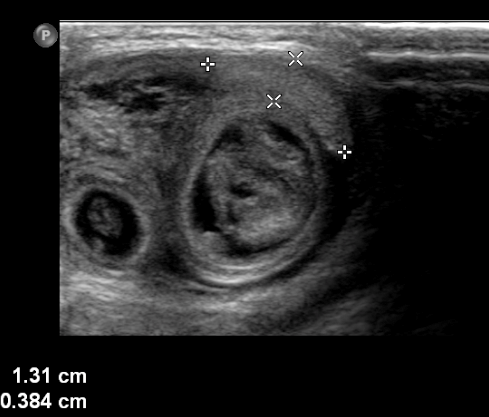
On initial evaluation he appeared nontoxic. Abdominal exam showed mild distension and possible guarding. Genitourinary exam revealed a non-tender, swollen right hemiscrotum that transilluminated, and a palpable right testicle. Given the concerning abdominal exam, a scrotal ultrasound was performed which showed loops of bowel, a hydrocele, and a right testicle with poor flow (Figure 1). After manual reduction was unsuccessful by the emergency physician and pediatric surgeon, the patient was urgently taken to the operating room. During laparotomy 10 centimeters of ischemic bowel was reduced and immediately regained perfusion. An ischemic testicle was also identified but not removed. Postoperatively, the patient was observed in the intensive care unit and was discharged on day four without complication.
Indirect inguinal hernias are the result of a patent processus vaginalis. They are common in preterm infants and must be considered in toxic neonates and those with scrotal swelling. Manual reduction is the preferred treatment but strangulated hernias must be surgically reduced.
 |
||||
| Figure 1. |
References:
Erdoğan D, Karaman I, Aslan MK, Karaman A, Cavuşoğlu YH. Analysis of 3,776 pediatric inguinal hernia and hydrocele cases in a tertiary center. J Pediatr Surg. 2013;48(8):1767-72.
Kumar VH, Clive J, Rosenkrantz TS, Bourque MD, Hussain N. Inguinal hernia in preterm infants (< or = 32-week gestation). Pediatr Surg Int. 2002;18(2-3):147-52.
Peevy KJ, Speed FA, Hoff CJ. Epidemiology of inguinal hernia in preterm neonates. Pediatrics. 1986;77(2):246-7.