

Originally Published: Common Sense, Winter 2011
Original Authors: Susan Cheng, MD MPH; Jonathan Yeo, MD; Eli Brown, MD; Allison Regan, MD
Edited by Michael C. Bond, MD FAAEM; and Alena Lira, MD
Testing of Low-Risk Patients Presenting to the Emergency Department with Chest Pain: A Scientific Statement from the American Heart Association. Amsterdam EA, Kirk JD, Bluemke DA , Diercks D, Farkouh ME, Garvey JL, Kontos MC, McCord J, Miller TD, Morise A, Newby LK, Ruberg FL, Scordo KA, Thompson PD. Circulation. 2010; 122: 1756-1776.
The American Heart Association (AHA) published a statement regarding the evaluation of low-risk chest pain in the ED ranging from assessing clinical symptoms to outpatient testing. There are over 8 million visits to the ED for chest pain every year in the United States with only a small percentage actually having a lifethreatening condition. At the same time, about 2% of patients with acute coronary syndrome (ACS ) are inadvertently discharged from the ED. The ED clinician must be able to determine when urgent therapy, admission and further testing, or direct discharge from the
ED is warranted.
Initial Assessment
Initial risk stratification is made by the ED clinician based on the history and physical, ECG, and cardiac injury markers. When symptoms are suggestive of ACS , patients may be deemed low-risk if they are hemodynamically stable, have no arrhythmias noted on telemetry, the ECG is normal, and the initial cardiac injury markers are negative.
Due to the wide differential of chest pain, the history should include questions to help determine the likelihood of ACS versus other causes of chest pain. The information obtained concerning the patient’s pain should include its location, onset, character, time course, severity, whether it radiates, any alleviating and/or exacerbating factors, history of similar episodes, and presence of any associated symptoms (e.g., diaphoresis, dyspnea, dizziness, palpitations, or nausea). Symptoms of myocardial ischemia are classically described as diffuse chest heaviness, pressure, or tightness that may radiate to the arm, neck, or jaw. However, careful attention should be made for atypical presentations known as “anginal equivalents” in certain populations such as the elderly, women and diabetic patients. These anginal equivalents include jaw, neck, or arm discomfort without chest pain; dyspnea; nausea; vomiting; diaphoresis; or fatigue. Sharp or stabbing pain may allude to pain that is musculoskeletal in nature. However, keep in mind that the Multicenter Chest Pain Study found that 22% of patients with sharp or stabbing chest pain were eventually diagnosed with ACS.(1)
A normal physical exam is found in the majority of chest pain cases. The exam can help identify higher-risk patients who might have signs of heart failure or peripheral arterial disease. The exam may also help suggest non-ACS causes of chest pain such as unequal extremity pulses (aortic dissection), prominent murmurs (endocarditis), friction rubs (pericarditis), fevers and abnormal lung sounds (pneumonia), or chest wall pain (musculoskeletal). However, any of these findings can be seen in a patient with ACS .
An initial ECG should be obtained within 10 minutes of presentation, as it is crucial in early risk stratification. In patients with a nonischemic ECG and no history of CAD, the frequency of MI was found to be 2% and 4% in those with a history of CAD. With a normal initial ECG, repeat ECGs have been recommended to assess for evolving ischemia. ST-segment depression (≥0.05mV) in contiguous leads, in the absence of LVH , is associated with an increased risk of ischemia. ECGs with posterior leads (V7-V9) or right-sided leads (V4R-V6R) may be done when suspicion of posterior or right-sided infarction is present.
Most patients with uncomplicated ACS have normal chest radiographs. Findings indicative of other diagnosis maybe noted on radiographs including widened mediastinum, enlarged cardiac silhouette, pleural effusion, pneumonia and pneumothorax.
Cardiac injury markers (highly sensitive and specific cardiac troponin) should be measured in all patients suspected of myocardial ischemia. In patients who present within 6 hours of symptom onset and with negative initial cardiac markers, the markers should be re-measured 6 to 8 hours after symptoms onset. Current troponin assays can identify most MIs within 3 hours of ED arrival. Because there are numerous non-ischemic causes of elevated troponins, confirmation of MI is based on the clinical setting and pattern of troponins. However, though a positive troponin can be diagnostic for myocardial ischemia, negative troponins do not equate to no ACS or myocardial ischemia.
Risk-scoring systems may help in risk stratification of chest pain. One simple criterion can be obtained with one set of cardiac markers, an ECG, and a history of CAD. If all three are negative, the patient can be considered low risk with a probability of MI <6%. The Thrombolysis in Myocardial Infarction (TIMI) score is widely used in high-risk patients but has shown mixed results when applied to lowrisk patients. The Global Registry of Acute Coronary Events (GRACE ) scoring system has been reported to be accurate in predicting risk, but is more complex than the TIMI score and many variables are not available in the ED. Scoring systems are recommended as adjuncts to clinical judgment in the evaluation of chest pain.
Chest Pain Units and Accelerated Diagnostic Protocols
Chest pain units (CPU) provide short-term observation of low-risk patients. They were created to carry out accelerated diagnostic protocols (ADP). ADPs provide cost-effective rapid assessment and exclusion of ACS in low-risk patients in order to prevent admissions and prolonged hospital stays. CPUs use ADPs to further stratify low-risk patients with serial ECGs and cardiac markers. If negative, further confirmatory testing is done to exclude inducible ischemia.
Confirmatory Test Selection in ADPs
The purpose of CPU observation and confirmatory testing in an ADP is to further minimize the likelihood of ACS low enough to warrant a safe discharge. Exercise treadmill testing (ETT) is the cornerstone of confirmatory testing in an ADP. The patient must be able to exercise and must have a normal baseline ECG. If the patient does not fit these criteria, an imaging test (myocardial perfusion imaging, echocardiogram, coronary angiography, or computed tomography coronary angiography (CTCA) may be considered. Historically, ETTs were done 48 hours after clinical stability but the AHA changed the recommendations in 2002 stating that ETTs should be done 6 to 8 hours after an evaluation that revealed no evidence of ischemia. Studies have shown the cost benefit of ETT in an ADP. One study of 421 patients showed no difference in cardiac events in 6 months in those managed with an ADP versus usual care, but the cost was 61% higher in the latter group.
Since many institutions are not able to provide confirmatory testing at all times, the American College of Cardiology (ACC )/AHA guidelines approve outpatient ETT in selected low-risk chest pain patients after a negative evaluation. The criteria include no further chest pain, non-diagnostic initial and follow-up ECGs, and normal cardiac injury marker measurements. A prospective study of 900 patients who underwent outpatient ETT had 3 nonfatal MIs and no deaths during follow up. This outpatient ETT should be obtained within 72 hours of their ED evaluation.
When ETT is not an option, the two most common stress imaging tests performed in CPUs are myocardial perfusion imaging (MPI) and echocardiography. They are both more accurate in detecting CAD than ETT, and they also provide information on left ventricular function as well as the location and extent of ischemia, if present. Stress imaging can be done with treadmill exercise as well as with pharmacologic agents such as dobutamine. MPIs can use coronary vasodilators such as dipyridamole or adenosine. Rest MPIs involve the injection of technetium 99m butilfenin radiopharmaceuticals. The technetium is taken up by the myocardium in direct relation to tissue perfusion and its redistribution is negligible, which makes it a good agent in the resting state. Because rest MPIs detect perfusion defects, old infarctions may also be seen on imaging. The rest MPI is beneficial because normal perfusion is associated with a very low clinical risk of ACS. Multiple studies have shown that rest MPIs can identify low and high-risk patients. Although MPI is associated with significant radiation exposure, they are a Class I indication in current guidelines for evaluation of patients with chest pain and non-ischemic ECGs.
Coronary artery calcification is considered a marker for CAD due to its relation with atherosclerosis. The coronary artery calcium (CAC ) score is a quantitative index of the extent of calcification measured by either electronic beam or multidetector computed tomography (CT). Studies have shown that a high CAC score is associated with an increased risk for coronary events and that a zero CAC score indicates a very low risk. A zero CAC score also has a negative predictive value close to 100% for early adverse events.
CTCA provides anatomic, rather than functional, information regarding coronary patency. With the advent of 64-slice multidetector CT scanners, major coronary arteries and branch vessels can be visualized. In a study of 368 patients, CTCA was found to have a sensitivity of 100% and a negative predictive value of 100% for ACS after 6 months of follow up. Compared with standard care, CTCA has been reported to decrease time to diagnosis (15 versus 3.4 hrs), the number of repeat evaluations for chest pain, and cost. However, several limitations do exist. About 25% to 50% of patients presenting to the ED with chest pain may not be candidates due to obesity, contrast allergy, intolerance to beta blockade, arrhythmia, renal insufficiency, or a history of CAD. Despite the limitations, CTCA has the potential for major clinical utility in the evaluation of low-risk patients in the ED due to its high negative predictive value (NPV).
Follow-Up of Patients with Negative CPU Evaluations
Most cases of chest pain with negative evaluations are non-cardiac in nature and require further evaluation for identification of the cause and management of their symptoms. Common causes of non-cardiac chest pain include pulmonary, gastrointestinal, musculoskeletal, or psychological causes. Panic attack or somatoform disorders may be causative factors in up to 40% of these patients. Finding a cause and managing symptoms will prevent unnecessary returns to the ED and improve quality of life. For patients with persistent concern even after negative noninvasive cardiac evaluation, coronary angiography or CTCA may be considered.
Can the HEART Score Safely Reduce Stress Testing and Cardiac Imaging in Patients at Low Risk for Major Adverse Cardiac Events? Mahler SA, Hiestand BC, Goff DC, Hoekstra JW, Miller CD. Critical Pathways in Cardiology 2011; 10: 1288- 133.
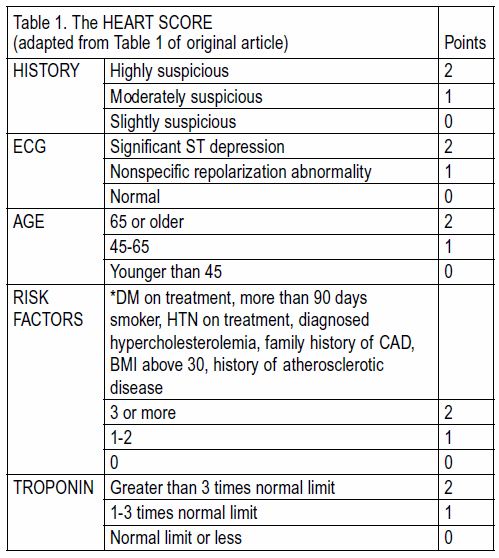
The authors conducted a cohort study to evaluate the ability of the HEART score, as a clinical decision aid, to safely reduce the need for objective cardiac testing in patients with low risk chest pain. The HEART score consists of: History, ECG, Age, Risk Factors, and Troponin (see Table 1). Low risk was defined as a score of 0-3 and high risk was a score of 4 or above. Prior clinical decision aids, such as the TIMI and GRACE score have lacked the sensitivity required to avoid the need for additional diagnostic testing or hospital admission. The primary outcome was a major adverse cardiac event (MACE ); defined as a composite end point of all-cause mortality, MI (defined as initial troponin greater than 1.0 ng/mL), or coronary revascularization during the index visit or within 30 days.
Patients were part of a registry of chest pain patients evaluated in the ED-based observation unit at Wake Forest Baptist Medical Center in North Carolina over a 28-month period between 2008 and 2010. The authors identified 1,070 low risk chest pain patients (mean age of 46.3 years old, 60.6% male, 56.5% Caucasian, 38.8% African American). To be included in the study population, low risk
was defined as chest pain patients with normal or non-diagnostic ECGs and negative initial cardiac biomarkers. HEART scores were determined for all patients in the registry using registry data and blinded chart review. Of the initial 1,070 patients deemed low risk, the HEART score categorized 84.5 % (904/1,070) as low risk and 15.5% (166/1,070) as high risk.
Of the 1,070 patients, 1.1% (12/1,070) had an index MACE . Cardiac testing (defined as stress test or cardiac imaging) was completed in 93.7% (1,003/1,070) patients. Record review for MACE was
completed on all registry patients and 30 day follow up data was available for 70% (753/1,070) of patients without index MACE . No additional MACE s were reported in the follow up data.
Patients with a low risk HEART score were significantly less likely to have a MACE than patients with a high-risk HEART score (0.6% vs. 4.2%, p<0.001). Using HEART would have resulted in 5 missed cases of ACS (a miss rate of less than 0.5%). Comparing the use of a high HEART score versus a TIMI score of <2 to assess for the need for further testing resulted in a potential reduction in cardiac testing of 84.5%. A high-risk HEART score was only 58.3% sensitive, and 85% specific for MACE . To improve the sensitivity and specificity, the authors combined HEART and use of 4-6 hour serial troponin. A high HEART score or a serial troponin greater than 0.065 ng/mL, resulted in 100% sensitivity and 83.1% specificity for a MACE with a potential cardiac testing reduction of 82.1%.
Analysis of the study reveals several limitations. The results may not be generalizable or reproducible. The HEART score needs to undergo external validation. The population was already preselected by the physicians’ decision to admit to the observation unit. Height and weight were not routinely recorded on registry patients, and thus body mass index (BMI) was not included as part of the HEART score calculation. Additionally, follow up data was only available for 70% of patients without an index MACE , and patients without complete follow up data were included in the final analysis as not having a MACE . Although promising, the use of the HEART score with serial troponin levels needs additional validation.
High-Sensitivity Troponin T Concentrations in Acute Chest Pain Patients Evaluated with Cardiac Computed Tomography. Januzzi JL, Bamberg F, Lee H, Truong QA, Nichols JH, Karakas M, Mohammed AA, Schlett CL, Nagurney JT, Hoffman U, Koenig W. Circulation 2010; 121:1227-1234.
For nearly twenty years, troponins have been the preferred cardiac biomarker for detection of myocardial injury. During this time period troponin assays have continued to evolve. Most recently, a new troponin assay has been developed which can detect changes in concentration of the biomarker at or below the 99th percentile for the normal population. The clinical utility of this new “high-sensitivity” troponin has been called into question due to its ability to detect very
minor degrees of myocardial injury, even in the absence of acute coronary syndrome (ACS ). This study used a high-sensitivity test for troponin (hsTnT) that used the 99th percentile cutoff and compared the hsTnT results with the clinical presentation and results of cardiac computed tomography.
The study participants were 377 low- to intermediate-risk patients who presented to the Massachusetts General Hospital ED between May 2005 and May 2007 with a chief complaint of chest discomfort. Exclusion criteria were as follows: elevated troponin on initial presentation, new ST depression or elevation on EKG, hemodynamic or clinical instability, known contrast allergy, serum creatinine >1.3 mg/dL, treatment with metformin, hyperthyroidism, inability to provide consent or perceived interference with standard clinical care of patients. Patients were followed for 6 months with an endpoint of a final diagnosis of ACS (unstable angina or acute MI). Charts were retrospectively reviewed by 2 physicians who were responsible for making the final diagnosis of ACS . Disagreement in the final diagnosis occurred in 4% of cases and was resolved by evaluation by a third reviewer.
Of the 377 patients, 37 (9.8%) were determined to have ACS and 25 of these were deemed to have unstable angina. Sixty-two of the 377 patients had an hsTnT > 13 pg/mL. Median concentrations of
hsTnT were found to be higher in patients with ACS and the highest in patients diagnosed with acute MI. Compared with cTnT, an hsTnT >13 pg/mL detected 50% more cases of ACS , and though more sensitive than cTnT, hsTnT was significantly less specific. Of the patients with hsTnT >13 pg/mL, 38 (62%) did not meet criteria for ACS . However, compared with patients without ACS and a negative hsTnT, patients with a high hsTnT were found to have higher incidence of cardiac abnormalities on CT angiography, such as larger cardiac chambers and increased left ventricular mass.
Based on the results above, the authors concluded that the hsTnT is more sensitive for detection of ACS than the cTnT in low- to intermediate-risk patients with chest pain. Furthermore they determined that patients with elevated hsTnT were found to have evidence of myocardial abnormalities on cardiac CT even in the absence of ACS , indicating that hsTnT may be a marker for cardiac structural disease and a sign of early myocardial injury. However, though the hsTnT was found to confer increased sensitivity for ACS when compared to conventional troponin, it was found to have a 10% reduction in specificity.
There are a few limitations to this study. The first is its small sample size, though a similar study by Reichlin which had a larger sample size yielded similar results.(2) A second possible weakness of the study is the timing of the hsTnT blood draw. Both the hsTnT and cTnT were drawn about four hours after presentation, at the same time as the CT angiography. It is possible that, had the samples been drawn earlier, the hsTnT may have proven less sensitive. Finally, only one set of cardiac markers was drawn, whereas serial measurements of troponins is standard of practice during evaluation for possible cardiac ischemia.
Though further research is needed regarding time to peak levels of hsTnT, and interpretation in patients with multiple medical comorbidities, the highly sensitive cardiac troponin has been proven
to be highly sensitive in the diagnosis of ACS . Interestingly, it may also provide insight into underlying cardiac disease, even in patients without ACS .
Utility of Absolute and Relative Changes in Cardiac Troponin Concentrations in the Early Diagnosis of Acute Myocardial Infarction. Reichlin T, Irfan A, Twerenbold R, Reiter M, Hochholzer W, Burkhalter H, Bassetti S, Steuer S, Winkler K, Peter F, Meissner J, Haaf P, Potocki M, Drexler B, Osswald S, Mueller C. Circulation. 2011 Jul 12;124(2):136-45. Epub 2011 Jun 27.
The purpose of this study was to determine the diagnostic accuracy of early absolute change versus relative change in high sensitivity cardiac troponin levels within the first 2 hours of presentation for the diagnosis of AMI in a nonselective heterogeneous population presenting with acute chest pain to the ED.
The Advantageous Predictors of Acute Coronary Syndromes Evaluation (APACE ) study is an ongoing prospective, international, multicenter study designed and coordinated by the University Hospital Basel in Switzerland. From 2006 to 2009, 1,247 consecutive patients were recruited (Caucasian, presenting to ED with symptoms suggestive of AMI who had onset of symptoms within last 12 hours). Dialysis patients and patients with ST elevation MI were excluded. All study patients received a standard assessment, initial troponin level and serial troponin levels as per the usual protocol at 6 to 9 hours as indicated. Additional highly sensitive troponin samples were collected on patients at 1 and 2 hours for study purposes. The study used both high-sensitive cardiac troponin T (hs-cTnT) and cardiac troponin I ultra (cTnI-ultra). Results were similar for both types of study troponin.
Of the remaining 1,197 patients, a 1-hour serial troponin was available for 836 patients, and 2-hour serial troponins were available in 590 patients. The outcome of interest AMI is defined as
evidence of myocardial necrosis with significant changes in troponin consistent with MI (at least one troponin value above the 99th percentile). The final diagnosis for each patient was determined by
two independent cardiologists blinded to the troponin measurements taken for study purposes from time of presentation to 60-day followup. Disagreement would be adjudicated in conjunction with a third cardiologist.
Of the 836 patients with 1-hour troponin levels, AMI was the final diagnosis in 108 patients (13%). Of the 590 patients with 2-hour troponin levels, AMI was the final diagnosis in 11%. Both the
absolute change and relative change between troponin levels at presentation and 1 hour and 2 hours were significantly higher in patients diagnosed with AMI (p<0.001). However, absolute change was superior to relative change in diagnostic accuracy using both 1-hour and 2-hour troponin levels for diagnosis of AMI (p<0.001). This diagnostic superiority was consistent in important subgroups such as the elderly and patients with impaired renal function. The diagnostic superiority of absolute over relative changes may be explained by the improved sensitivity of the troponin assays to detect very small changes, and patients presenting several hours after onset of symptoms will already have elevated baseline troponin levels and thus will not be able to mount a significant relative increase.
In addition, the combined use of elevated baseline troponin and early absolute changes resulted in a significant improvement of diagnostic accuracy for AMI for hs-cTnT (p=0.001 for 1 hour, p<0.001 for 2 hour absolute change), and improved, but less significantly for cTnI – ultra (p=0.05 for 1 hour, p=0.02 for 2 hour absolute change). The analysis also revealed that 1- or 2-hour absolute change in troponin levels was as good as a 6-hour serial troponin level for diagnosis of AMI. Lastly, statistical analysis reveals the optimal cutoff for the 2-hour absolute troponin changes were approximately half of the 99th percentile value of their respective assay. These results suggest that the traditional threshold of above 99th percentile is no longer needed to diagnosis AMI using these new assays.
This study is limited because it was an observational study and we can only infer the potential impact of study troponins had they been used to determine clinical care. There was an inherent bias
in the group with 6-hour troponins, because most patients with AMI would have already been transferred to cardiac catherization lab. In addition, this study excluded dialysis patients. Despite these limitations, the conclusions from this study regarding early absolute troponin level changes could greatly impact ED evaluation of chest pain patients.
Estimating the Clinical Impact of Bringing a Multimarker Cardiac Panel to the Bedside in the ED. Birkhahn RH, Haines E, Wen W, Reddy L, Briggs WM, Datillo PA. Am J Emerg Med.
2011 Mar;29(3):304-8. Epub 2010 Apr 2.
The authors of this prospective study investigated whether implementing point-of-care (POC) testing of cardiac biomarkers would decrease the amount of time necessary to risk stratify patients with chest pain in the ED.
Adults greater than 18 years old being evaluated for suspected ACS were approached for enrollment in this prospective study, as long as the initial ECG showed no ST-segment elevation. Enrolled patients were immediately tested for cardiac markers, both core laboratory TnT and a POC multimarker. They were then retested with the POC multimarker at 2 hours, and the core laboratory TnT at 6 hours. The POC multimarker chosen for the study included TnI, myoglobin, and creatinine kinase MB.
The study enrolled 151 patients, all of whom had both the accelerated POC pathway and the standard 6-hour TnT interval testing. The standard core laboratory pathway identified 12 patients with elevated TnT, and all of them were also identified via the accelerated pathway. The POC pathway also had 48 false-positive elevations (32%), which were confirmed by negative TnT enzyme levels at 6-hours. Based on these results, a positive predictive value of the POC pathway was calculated to be 20%, with a negative predictive value of 100%.
The average time for the 2nd POC test to become available was 270 minutes, compared to 660 minutes for the 2nd TnT result. The average time savings from implementing a POC cardiac pathway
was calculated to be 390 minutes (6.5 hours), 4 hours of the 6.5 hours time saved can be explained from use of the accelerated pathway and the remaining 2.5 hours saved is from bringing the test to the bedside. The average 390 minutes per patient time savings was then compared to the cost of implementing a more expensive accelerated cardiac pathway. Using a theoretical ED with 70,000 annual visits, 5% of which are evaluated for ACS using serial cardiac biomarker measurements, it was projected that this intervention would provide a savings of 13,650 direct patient care hours in the ED per year. After estimating an incremental cost of $100,800 per year to implement the rapid acute cardiac evaluation pathway, it was calculated to cost $7.40 for every hour of direct patient care saved.
Patients with suspected ACS have traditionally been admitted to the hospital for cardiac monitoring and serial cardiac biomarker measurements after one blood draw. It has been proposed that
with better risk stratification fewer patients would require telemetry admissions. This study shows that trending cardiac biomarkers via an accelerated pathway utilizing a bedside multimarker approach could save an average of 6.5 hours per patient suspected of having ACS . Though more expensive, it is presumed that the direct cost of the strategy would be more than offset by a reduction in patient workload, increased utilization of the same ED bed, as well as patient satisfaction by more efficiently risk stratifying patients to an appropriate level of care.
This study was limited by a relatively small number of patients and a single ED experience. Furthermore, other EDs may not experience the same delay in obtaining the 6-hour TnT lab results. The study also does not take into account that 32% of the POC testing demonstrated false positive results, which would either increase the number of admissions to telemetry or decrease in the amount of time-savings by requiring a confirmatory 6-hour TnT test. This study also does the address the need for a provocative test to evaluate for inducible myocardial ischemia.
Coronary Computed Tomography Angiography for Early Triage of Patients with Acute Chest Pain: The Rule Out Myocardial Infarction using Computer Assisted Tomography (ROMICAT ) trial. Hoffmann U, Bamberg F, Chae CU, Nichols JH, Rogers IS, Seneviratne SK, Truong QA, Cury RC, Abbara S, Shapiro MD, Moloo J, Butler J, Ferencik M, Lee H, Jang IK, Parry BA, Brown DF, Udelson JE, Achenbach S, Brady TJ, Nagurney JT. J Am Coll Cardiol. 2009 May 5;53(18):1642-50.
Coronary computed tomography angiography (CCTA) is a test that can rapidly and accurately visualize significant coronary artery stenosis and coronary atherosclerotic plaques. The relationship between such findings and acute coronary syndrome, however, has not been established. The authors of this observational study investigated the utility of CCTA in assessing patients with low to intermediate risk for ACS who present to the ED with acute chest pain.
This was a prospective observational cohort study of patients without established CAD who presented to the ED with a chief complaint of acute chest pain for greater than 5 minutes during the last 24 hours. All patients had a normal initial troponin and an ECG that was negative for ischemic changes. If enrolled, patients underwent a contrast-enhanced CCTA prior to admission to the hospital floor using a 64-slice CT scanner. Images were reconstructed and read by 2 experienced investigators in search of coronary plaque and stenosis. Significant stenosis was defined as a luminal narrowing greater than 50%. If a consensus was not reached, a third expert reader made the final diagnosis. All physicians caring for the patient remained blind to the result of the CCTA. The two clinical endpoints established for the study included ACS during hospitalization and MACE within the 6-month follow-up.
The study enrolled 368 patients, of which 31 were diagnosed with ACS . Of the 337 subjects without ACS , zero suffered a MACE at 6 months. Of the 368 enrolled subjects, 183 were found to have no CAD by CCTA or ACS giving the test a negative predictive value of 100% when completely negative. A plaque with no significant stenosis was found in 117 patients, and 34 were read as positive for stenosis greater than 50%. The specifics of finding plaque and significant stenosis on CCTA were calculated to be 54% and 87% respectively for ACS .
This study demonstrates that CCTA can be utilized for ruling out ACS in low-risk patients presenting with acute chest pain. In the future CCTA may also improve management of acute chest pain as the presence and extent of CAD is considered a powerful predictor of future cardiovascular events. The strength of CCTA, however, is the high NPV for ACS and the fact that half of the patients in the studied population had no CAD detected. Low risk chest pain patients with a negative CCTA can be directly discharged from the ED without further diagnostic testing or hospital admission.
One restraint to this approach in low risk chest pain patients is the associated radiation exposure and its potential long-term affects. The study has limited generalizability because it was at a single center, had a dedicated research team who performed the CCTA exams, and highly experienced personnel to interpret the images. Nonetheless, lack of plaque and stenosis on CCTA can negatively predict ACS independent of cardiovascular risk factors or TIMI risk score. Given the large number of patients with low to intermediate risk of ACS presenting to the ED with chest pain, early CCTA has the potential to significantly improve patient management in the ED.
Coronary Disease in Emergency Department Chest Pain Patients with Recent Negative Stress Testing. Walker J, Galuska M, Vega D. West J Emerg Med 2010;11 (4): 384-388.
Chest pain accounts for 5% of emergency department visits in the United States and represents the second most common presenting complaint. The decision by an ED physician to admit or discharge a patient with chest pain can be a difficult one, which often relies on risk stratification. Despite this, one study by Pope et al. found that ED physicians discharged home 2.1% of acute myocardial infarctions and 2.3% of patients with unstable angina.
This disposition decision can be further complicated in the setting of a patient who has had a recent negative stress test. Depending on the study and the type of stress test, the sensitivity and specificity of cardiac stress tests for diagnosing coronary artery disease range from 67-85% and 70-95%, respectively. This study sought to determine the likelihood of adverse cardiac events in patients with recent negative stress tests.
This study is a retrospective chart review of patients with a presenting chief complaint of chest pain that have undergone a negative cardiac stress test within the last three years. Charts were reviewed for adverse cardiac events in the 30 days after ED presentation.
The study was performed at a community teaching hospital with 70,610 ED visits in 2007, 7.9% (5,591) of which were for chest pain. For patients with multiple ED visits for chest pain, each visit was counted as a separate entry in the study. For patients who have undergone multiple stress tests, only the results from the most recent stress test were included. Of note, stress tests that were reported as inconclusive because the patient did not reach the 85% maximum heart rate target were included in the study and considered equivalent to a negative test.
Of the 337 charts reviewed, 164 patients met inclusion criteria. Forty-two of these patients had an inconclusive, rather than a negative, stress test. While the majority of patients had a treadmill echocardiogram, other types of stress tests such as pharmacological echocardiograms, pharmacologic nuclear studies, treadmill nuclear studies and a treadmill ECG study were included as well. Of the 164 patient encounters reviewed, 34 had significant CAD within 30 days following admission. Significant CAD was defined as a myocardial infarction with positive cardiac markers, positive stress test, cardiac catheterization requiring intervention (angioplasty or medical management), CABG or death due to non-traumatic cardiac arrest. Of note, 25 of the 122 patients who had a negative stress test had CAD, while 9 of the 42 patients who had an inconclusive stress test had CAD. Based on this data, the authors concluded that a prior negative stress test should not be used to definitively rule out CAD.
There were several limitations to this study that deserve mentioning. The first is inherent in the study’s design as a retrospective chart review with a relatively small sample size. Also, the fact that it was performed at a single institution makes it possible that results may not be entirely applicable to other populations. Furthermore, as only admitted patients were included, the study results are biased towards a population which is more likely to have a higher rate of significant CAD when compared to patients who were discharged from the ED. Finally, chart reviewers were not blinded to the study’s purpose.
This study found that 20.7% of patients presenting to the ED with chest pain who had negative cardiac stress testing within the prior 3 years suffered a significant cardiac event in the 30 days after admission. This percentage is significantly higher than a similar study by Nerenberg in which CAD was found in 5.2% of patients with a recent negative stress test.(3) However, the authors in this study attributed this difference to the inclusion of both admitted and discharged patients in the other study. This discrepancy, in addition to the limitations outlined above, demonstrates the need for additional research on this subject. The major take home point is that a negative stress test does not mean the patient does not have CAD. Even if you use the Nerenberg study which showed that only 5.2% of patients with a negative stress test had CAD, that means you will be sending home 1 in 20 patients that can have an MI. Future research should include a larger sample size and may consider distinguishing between different modalities of cardiac stress testing.
References:
1. Lee TH, Cook EF, Weisberg M, Sargent RK, Wilson C, Goldman L. Acute chest pain in the emergency room: identification and examination of low-risk patients. Arch Intern Med. 1985;145:65-69.
2. Reichlin T, Hochholzer W, Bassetti S, Steuer S, Stelzig C, Hartwiger S, Biedert S, Schaub N, Buerge C, Potocki M, Noveanu M, Breidhardt T, Twerenbold R, Winkler K, Bingisser R, Mueller C. Early diagnosis of myocardial infarction with sensitive cardiac troponin assays. N Engl J Med. 2009;361:858-867.
3. Nerenberg RH, Shofer FS, Robey JL, Brown AM, Hollander JE. Impact of a negative prior stress test on emergency physician disposition decision in ED patients with chest pain syndromes. Am J of Emerg Med. 2007;25:39-44.