
 |
| Image Credit: Flickr |
Author: Jennifer Reink, MSIV
Ohio University Heritage College of Osteopathic Medicine
AAEM/RSA Social Media Committee ’16-’17
 |
| This post was peer reviewed. Click to learn more. |
With school back in session and autumn just around the corner, the fall sports season is upon us, and where there are athletic competitions, there are bound to be concussions. Nearly half of all emergency department (ED) visits for concussions are sports related, with 4 in 1000 children ages 8 to 13 and 6 in 1000 children ages 14 to 19 presenting to the ED each year for a concussion sustained during an organized team sport.[1] Furthermore, sports are second only to motor vehicle accidents as the leading cause of traumatic brain injury among people ages 15 to 24.[2] From football and cheerleading, to swimming and basketball, each sport has its own risk for head injury. For those of us who find ourselves caring for these young beaten warriors, here is what you need to know about what makes sports-related concussions such a challenging diagnosis.
1) Clinical symptoms are often subtle and may manifest with immediate or delayed onset.
A concussion is defined as a disturbance in brain function caused by a direct or indirect force to the brain resulting in a disruption of neural membranes.[1,3] This leads to a variety of non-specific signs and symptoms. Although symptoms typically present immediately after injury, some may not appear until several hours following impact. There are even patients who present days later with delayed or worsening symptoms. Common manifestations of concussions include:[2,3]
- Headache (most common)
- Nausea or vomiting
- Dizziness or unsteadiness
- Blurry or double vision
- Fatigue or drowsiness
- Change in sleep pattern
- Sensitivity to light or noise
- Difficulty concentrating or remembering
- Depression
- Nervousness, sadness, or irritability
- Feelings of being “off” or “foggy”
- Unusual behavior
- Seizures
- Amnesia
- Loss of consciousness (occurs in <10%)
2) Cognitive function and balance impairment may be helpful in diagnosis during the first 24 hours, but often normalizes within a few days.
Unfortunately, there are few objective findings for diagnosis. Some forms of evaluation like the Sport Concussion Assessment Tool or SCAT3 are becoming more widely utilized by school and athletic associations and may provide physicians with an athlete’s baseline level for comparison.[4,5] Medical evaluation should include a thorough history of the event, neurological exam, and cognitive screening comprised of vision, hearing, strength, sensation, balance, coordination, reflex, memory, concentration, mood, and recall assessments.[3,4,5]
3) Physical and cognitive exams are often completely normal and additional tests such as CT, MRI, and blood tests are non-diagnostic.
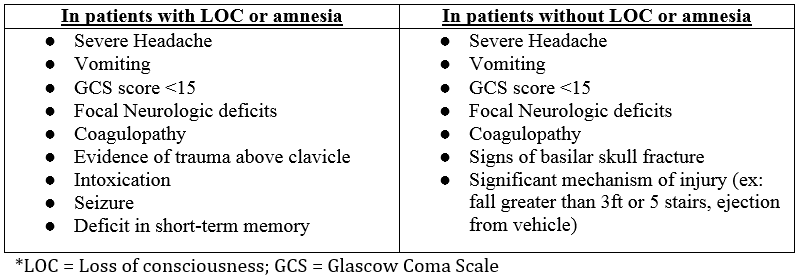
The use of CT scanning for patients with suspected concussions continues to be controversial. However, a CT may be considered if a patient has worsening headache, becomes drowsy, has repeated vomiting, lethargy, or hard neurologic symptoms that raise concern for a skull fracture, cervical spine injury, epidural or subdural bleed.[3,6,7] Risk factors for imaging should always be discussed with patients and their parents to allow for an informed decision and avoidance of unnecessary radiation.
Imaging is generally indicated if patients have at least one or more of the following:[6]
4) Current treatment recommendations encourage complete physical and mental brain rest.
Some general advice for patients includes:[2,3,5]
- Avoiding visual and sensory stimuli including reading, watching TV, or using a computer
- Avoiding strenuous mental tasks including homework
- Eating well-balanced meals
- Avoiding activities that could lead to further head injury
- Avoiding alcohol
- Avoiding airplane flights shortly afterward due to potential for worsening symptoms
- Avoiding tiring activities like heavy cleaning, exercising, or playing video games
- Easing into normal activity slowly
- Being re-evaluated and cleared by a primary care physician before resuming activities including driving, sports, work, school, and play
Once a diagnosis is made, acetaminophen is the most commonly recommended agent. Other medications may be indicated for specific symptomatic relief. Most concussions resolve spontaneously within seven to 10 days with symptoms typically lasting less than 72 hours.[3]
5) Athletes may under-report symptoms or exaggerate their level of recovery in hopes of being cleared to compete more quickly.
Many athletes (and their parents) will be eager to know when they can return to athletic activities. Modifying factors and co-morbidities including Attention Deficit Hyperactivity Disorder (ADHD), migraines, learning disabilities, and mood disorders should be considered when making the diagnosis, devising management plans, and in making both return to play and return to learn recommendations.[5] Before returning to a normal routine, a patient must be completely symptom-free and have returned to his or her concussion baseline scores (when available). Patients should then start a five-day program in which they gradually increase activity while being monitored closely for return of symptoms.[5]
Concussions continue to be a common cause of emergency department visits, especially among children and athletes. With the Summer Olympics in our not so distant past, we may see an increase in sports related injuries this fall as more children enroll in athletics in hopes of becoming the next Simone Biles or Michael Phelps. By understanding the basics of concussion presentation, assessment, and treatment, we can help athletes of all ages safely train, play, and compete.
References:
- Bakhos LL, Lockhart GR, Myers R, Linakis JG. Emergency department visits for concussion in young child athletes. Pediatrics. 2010;126(3):550-556.
- Halstead ME, Walter KD. American Academy of Pediatrics. Clinical report–sport-related concussion in children and adolescents. Pediatrics. 2010;126(3):597-615.
- Scorza, KA, Raleigh, MF, O’Connor, FG. Current concepts in concussion: evaluation and management. Am Fam Physician. 2012:85(2):123-132.
- SCAT3. Br J Sports Med. 2013;47(5):259.
- Concussion guidelines: diagnosis and management of sport-related concussion guidelines. National Collegiate Athletic Association Web site. http://www.ncaa.org/health-and-safety/concussion-guidelines. Updated 2015. Accessed August 24, 2016.
- Zonfrillo MR, Kim KH, Arbogast KB. Emergency Department Visits and Head Computed Tomography Utilization for Concussion Patients From 2006 to 2011. Acad Emerg Med. 2015;22(7):872-7.
- Lovato, LM. Identifying and treating concussion. Emergency Medicine News. 2010;32(3);18-19.