
 |
| Image Credit: Wikimedia |
{kind=link}
 |
| This post was peer reviewed. Click to learn more. |
Author: Alfred Morrobel, M.D
Universidad Iberoamericana
Epidemiology
Congestive heart failure (CHF) in children is diverse due to the myriad underlying etiologies that can occur from birth to adolescence. In the United States, CHF is estimated to affect 12,000 to 35,000 children below the age of 19 years and there are approximately 11,000 to 15,000 heart failure-related hospitalizations in children per year.[1]
Pathophysiology
Pediatric CHF is divided into three pathophysiologic categories:[2]
- Primary ventricular pump dysfunction is the most prevalent and usually occurs in children with preceding infections, genetic predispositions, or medication-induced cardiotoxicity. Cardiomyopathies are among the most common causes of ventricular pump dysfunction, in which the estimated incidence of pediatric cardiomyopathy in the US is approximately 1 case per 100,000 children per year, due to mostly dilated cardiomyopathy.[3]
- Volume overload with preserved ventricular contractility is due to an abnormally structured heart due to congenital heart defects (CHD) such as ventricular septal defect (VSD), patent ductus arteriosus (PDA), atrial septal defect (ASD), atrioventricular septal defect, and others. These are second only to cardiomyopathy.[3]
- Pressure overload with preserved ventricular contractility is due to ventricular outlet obstructions (aortic stenosis, pulmonary stenosis), and is the least likely to cause pediatric CHF.[3]
Signs and Symptoms
Physicians in the emergency department (ED) must recognize pediatric CHF and the different clinical manifestations depending on the age of the patient. In general, the symptoms are similar to those of an adult with CHF, such as easy fatigability, exercise intolerance, dyspnea with effort or at rest, hepatomegaly, and syncopal episodes.[3] However, based on whether the patient is an infant, child, or adolescent, other significant symptoms are varied (Table 1).[4]
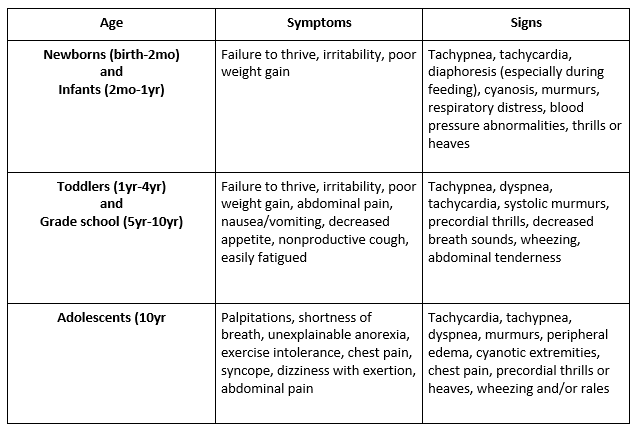 |
| Table 1: Signs and Symptoms of Pediatric Congestive Heart Failure by Age |
Remember, too, that vital signs will vary greatly by age. See Table 2.[5]
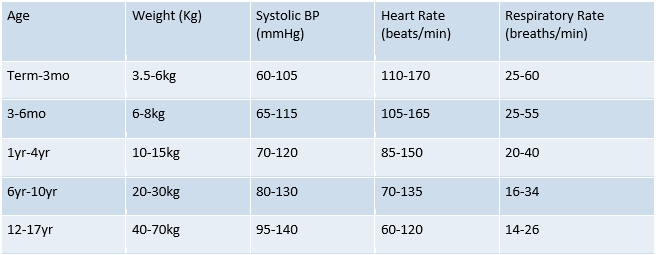 |
| Table 2. Normal Pediatric Vital Signs |
ED Management of Acute CHF
As with any emergent case, focus on airway, breathing, and circulation, including intubation as indicated and intravenous (IV) access.
- Airway
- Consider positive pressure ventilation (invasive or noninvasive) to offload left ventricle work, but proceed cautiously if you do not know the structural defect since positive pressure can worsen right ventricular function.[7]
- 100% FiO2
- Breathing
- Carefully evaluate the patient’s work of breathing. Though the patient’s arterial blood gas may not be significantly abnormal, the patient may still fatigue and decompensate.
- As in adults, start a nitroglycerin infusion for severe CHF with pulmonary edema to vasodilate pulmonary vasculature.[8] If the patient appears volume-overloaded, give a loop diuretic, such as furosemide (Lasix) or bumetanide (Bumex). This is to offload the left ventricle, which may be responsible for pulmonary edema.[6]
- Circulation
- IV access
- EKG: Look for arrhythmias (such as long QT, atrial fibrillation, heart blocks) and suggestion of structural disease (such as left ventricular hypertrophy).
- Afterload reduction is critical to improving circulation. If you have not started a nitroglycerin infusion for pulmonary edema, start a nitroprusside or nicardipine infusion to reduce the afterload, which reduces the necessary work of the heart, improving cardiac output.[8] Although there is limited evidence in pediatrics, afterload reduction with an angiotensin converting enzyme (ACE) inhibitor can improve cardiac output in patients who do not warrant infusions.[7] Be very cautious, though, because the effects of ACE inhibitors can last several hours.
- Give inotropic support if the blood pressure is too low. Digoxin remains a key drug for pediatric patients, but takes 12-24 hours to fully take effect. Dopamine remains the most commonly used inotrope for pediatric heart failure patients in the emergent setting, followed by dobutamine. Epinephrine and norepinephrine are typically only used postoperatively.[8]
- Extracorporeal membrane oxygenation (ECMO) can be lifesaving in children who are unresponsive to medical therapy.[7] Mechanical circulatory support (MCS) maintains end-organ function and reduces myocardial oxygen requirements. In a report from the International Society for Heart and Lung Transplantation (ISHLT), one-third of pediatric heart transplant recipients received MCS as a bridge to transplantation.[7]
Conclusion
It is vital to recognize pediatric CHF because it can lead to rapid complications if treated incorrectly. It differs from adult CHF primarily in etiology, as well as in clinical presentation. Signs and symptoms differ amongst children of different age groups, and time of onset of CHF is important in making the diagnosis. Management in the ED begins with stabilization of the patient, focusing on airway, breathing, and circulation. Further management includes EKG, afterload reduction, and positive inotropes. Lastly, ECMO/MCS is reserved for those unresponsive to medical therapy. The overall outcome with CHF is better in children than in adults, as it is commonly due to structural heart disease and reversible conditions which are amenable to appropriate therapy.
References:
3. Talner N. Heart failure. Heart Disease in Infants, Children, and Adolescents. 1995:1746-73.
5. Fleming S, Thompson M, Stevens R, et al. Normal ranges of heart rate and respiratory rate in children from birth to 18 years of age: a systematic review of observational studies. Lancet 2011; 377:1011.
6. Erickson LC. Medical issues for the cardiac patient. Critical Care of Infants and Children. 1996:259-62.
8. Sharma M, Nair MNG, Jatana SK, Shahi BN. Congestive heart failure in infants and children. Med J Armed Forces India. 2003;59(3):228-233.