
 |
| Photo by NEC Corporation: https://flic.kr/p/nJ7P9M |
Author: Andrew W Phillips, MD MEdStanford/Kaiser Emergency Medicine Residency Program
You will be judged by your consultations. Period.
The best evidence we have for handling emergency department (ED) consultations supports the use of the “5 C’s of consultation,” which was shown to be helpful in a randomized, controlled trial.[1]
1) Contact: start with an introduction between you and the consultant.
2) Communicate: provide a concise story.
3) Core question: have a specific question or request for the consultant (“What do you think is wrong?” is unacceptable).
4) Collaboration: create agreement between you and the consultant about further management by the emergency department and the consulting team.
5) Closing the loop: ensure you and the consultant have the same plan.
Within the core question components, it is also important to know and express to the consultant the goal of the consultation. There is a taxonomy of consultations with differing goals, which can be divided into: [2]
a. Immediate critical intervention (e.g., stroke code)
b. Procedural (e.g., anesthesia for a blood patch)
c. In-person evaluation and management (e.g., admitting neutropenic fever)
d. Remote evaluation and recommendations (e.g., neurosurgery evaluation of a CT scan remotely)
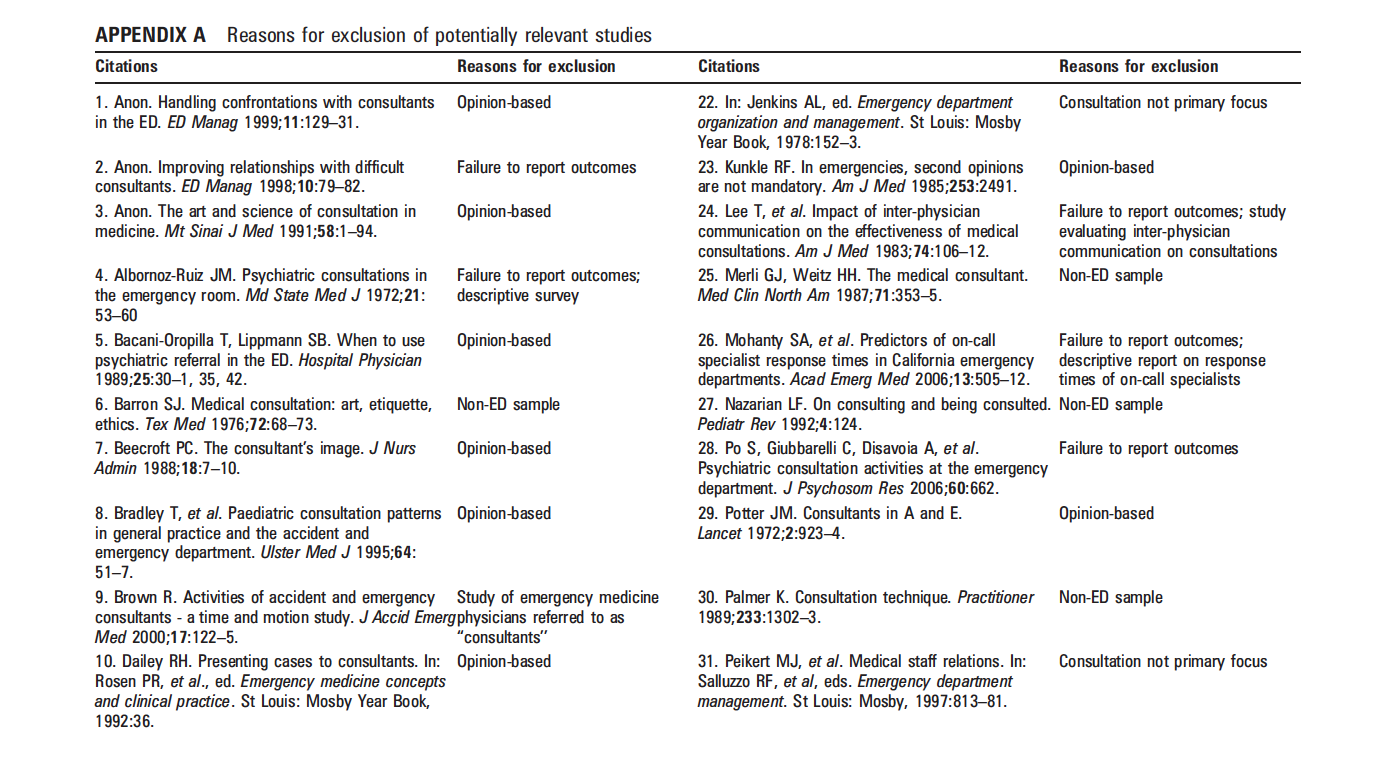
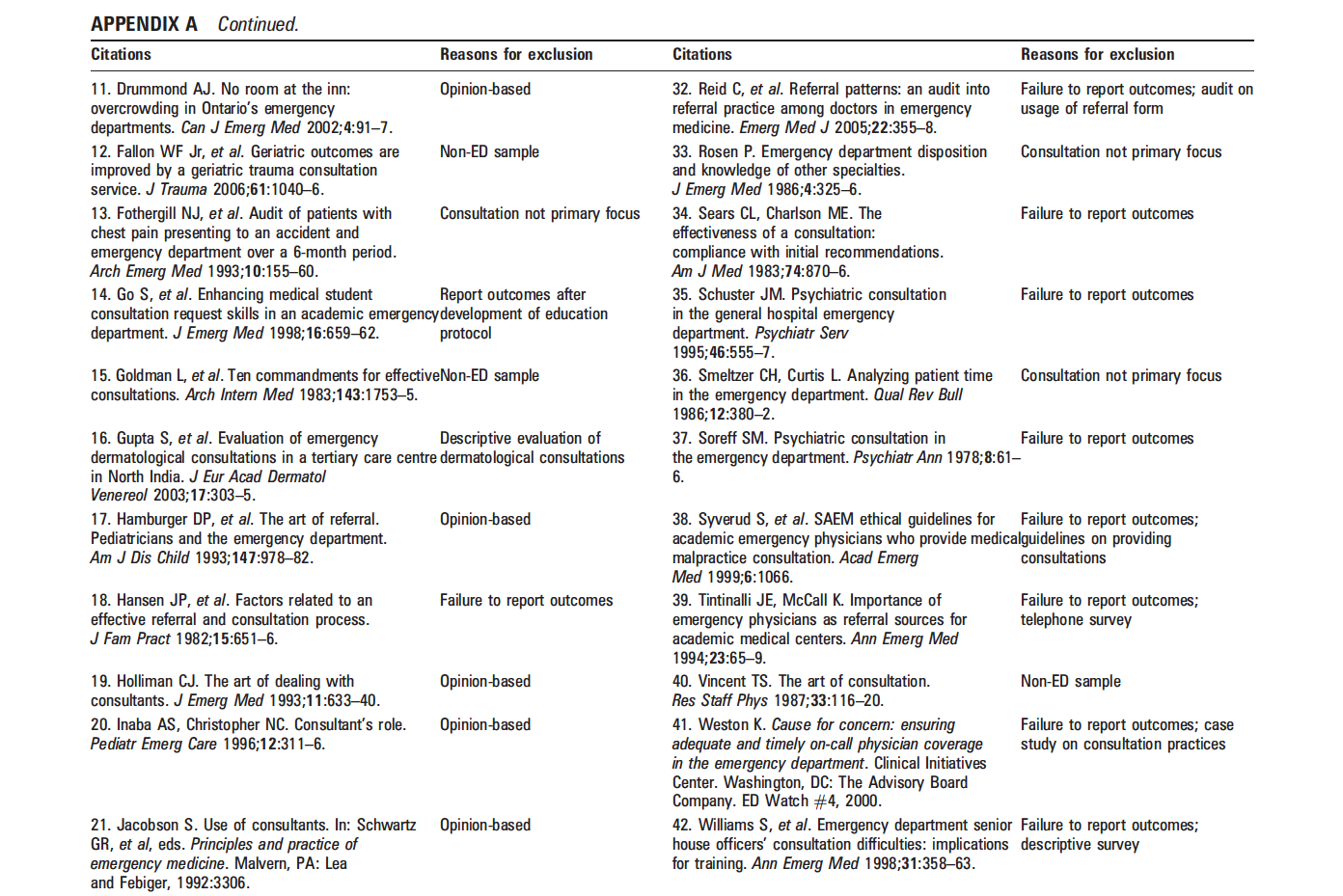
Appendix A of a review article in the Emergency Medicine Journal contains a nice list of articles that were excluded from their review for various reasons.[3] The list doubles as a good list of opinion articles on the topic; Holliman’s article is especially valuable.[4]
 |
| Click to enlarge |
 |
| Click to enlarge |
This advice basically comes down to: put yourself in the shoes of a tired, overworked consultant who is being given more work by the ED, and ask yourself what sort of interaction you would want. You would want the patient worked up fully, stabilized as much as possible, and at least actively receiving the first round of treatment. Here are some suggestions that are not evidence based but can make life better for you:
- Ask the consultant’s name as soon as they answer. They’re not going to want to give you their name at the end of the conversation if it became an aggressive conversation. Also, if you are a medical student, do NOT tell them you are a student. You’re just “John Doe” from the ED. If they ask, don’t lie, but you don’t have to offer that information up front.
- Weigh carefully the balance between freeing up ED beds and having things fully prepared for the consultant. Use ED resources to your advantage. For example, ask the ED clerk to get patient records from an outside facility or enter into the system the various contact numbers for family members of the demented patient. Make sure to mention such efforts to the consultant: “I wanted to help you out, and we already have a request in for the records,” or something like that. There is a fine line between helping out and being run over, so toe it carefully.
- Don’t be above bribery. I routinely bring 4-5 chocolates with me on shifts and pass them out to consultants when I see them, always saying “Thanks for taking care of Mrs. X.”
- Although the 5c’s start with the story, I find it helpful to jump to the punch line so the consultant can hear the story in the context of the goal. For example, I called a consultation last night like this: “Hi, Dr X, thanks for calling back. I have a pleasant 80 year old female with a pneumonia who CURB’s out (CURB-65) to 13% (mortality) and new subtle heart failure who didn’t fly with an ambulation trial. She presented with…” Now the consultant knows the diagnosis and that she needs to be prepared to admit the patient.
- Gently express your desire for admission. Notice in the example above that I didn’t say “You need to admit the patient.” I phrased it as “the patient CURB’s out” and “isn’t flying.” Obviously if the patient has a 13% chance of dying, she can’t go home. When I said “didn’t fly” that also demonstrates that we “road tested” her, so to speak, and she failed. She was short of breath walking. Can’t walk = can’t go home. Consultants don’t want to be told what to do, but they can read between the lines.
- Finally, don’t get trapped into their sense of time. Your time is valuable. If they start asking you to read the medication list to them, politely say, “Good question, we’ve updated the medication list” (if you did) or “the patient has a med list at bedside,” or something like that. And add, “it will be faster if you take a look at that.” If that doesn’t work you can excuse yourself with, “I’m sorry, but I need to take care of another patient. I’m happy to speak with you when see the patient. Thank you for your time.”
Practical Example
- “ED, this is Andrew Phillips” (first and last name, professional)
- “Surgery, I was paged.”
- “Thanks for calling back (being polite), with whom am I speaking?”
- “Sam.”
- “Thanks, Sam. Patient’s medical record is 123456789. (Lead with identifying information so they can look up the patient while you talk.) I’m calling for your clinical recommendation for OR versus CT scan (clear question) on a 6 year old male potential appy (speak their language). He has 2 days progressive right lower quadrant pain and an ultrasound that couldn’t see the appendix. Also decreased appetite, fever of 39 without leukocytosis yet (frame the story as you see it progressing). He’s in Bed 3.” (Read that out loud and it will be about a 30 second monologue.)
- “Last meal?”
- “6 hours ago.” I’m pretty sure he’s going to the OR so I prepared the consent form to help you out (shows that you care). Anything else you recommend at this time?” (Not important enough information to put in my introduction but I have the information prepared.)
- “Can we get a pro-calcitonin?”
- “Sure, that’s reasonable. You’ll press on his belly and let me know if you want to go straight to the OR or get a CT scan?” (closing the loop)
- “Yeah.”
That’s it. Look back and you’ll see that each of the 5 c’s were included, and the whole thing took one minute. One last piece of advice: write the name of the consultant and time of the discussion in the chart. If anyone has questions later about who said what and when, you’re covered. Now you’re off to see your next patient!
References
1. Kessler CS, Afshar Y, Sardar G, Yudkowsky R, Ankel F, Schwartz A. A prospective, randomized, controlled study demonstrating a novel, effective model of transfer of care between physicians: the 5 Cs of consultation. Acad Emerg Med. 2012 Aug;19(8):968–74.
2. Kessler CS, Asrow A, Beach C, Cheung D, Fairbanks RJ, Lammers JC, et al. The taxonomy of emergency department consultations–results of an expert consensus panel. Annals of Emergency Medicine. 2013 Feb;61(2):161–6.
3. Lee RS, Woods R, Bullard M, Holroyd BR, Rowe BH. Consultations in the emergency department: a systematic review of the literature. BMJ: British Medical Journal. 2007.
4. Holliman CJ. The art of dealing with consultants. The Journal of Emergency Medicine. 1993 Sep;11(5):633–40.