

 |
| This post was peer reviewed. Click to learn more. |
Author: Ashley Grigsby, DO, PGY-4
Combined Emergency Medicine/Pediatrics
Indiana University
Case
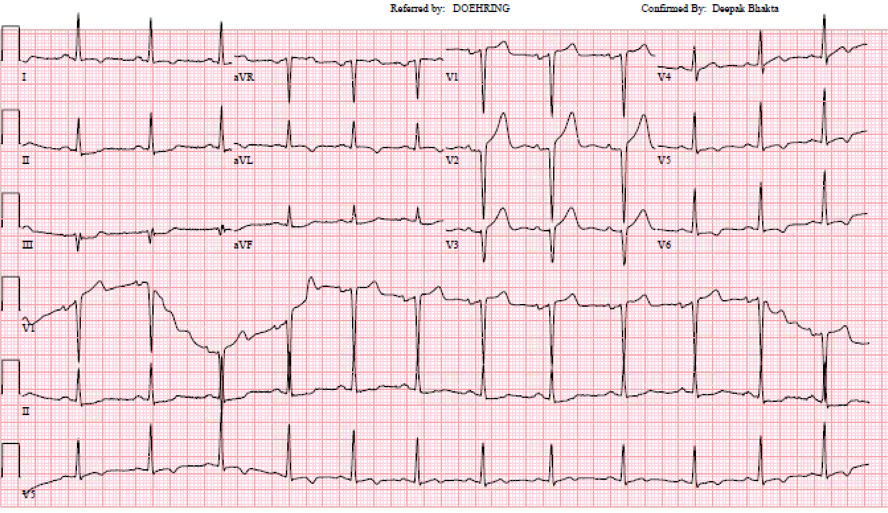
A 32-year-old previously healthy African American male presents via emergency medical services (EMS) for evaluation of chest pain. An ST elevation myocardial infarction (STEMI) code had been activated by EMS based on pre-hospital electrocardiogram (EKG) that had been interpreted as ST elevation in the anterior leads with reciprocal ST depression in the lateral leads. On arrival to the emergency department (ED), the patient appears ill and reports severe crushing chest pain radiating to the arm and down into the abdomen. He is diaphoretic and clutching his chest. His heart rate is 123 beats per minutes, respiratory rate 16 breaths per minute, and blood pressure 210/110 mmHg. He is afebrile. Initial ED EKG is shown below.
Questions
- How should this EKG be interpreted?
- Should this patient be sent to the catheterization lab under STEMI activation?
- What other testing should be considered in this patient?
Case Outcome
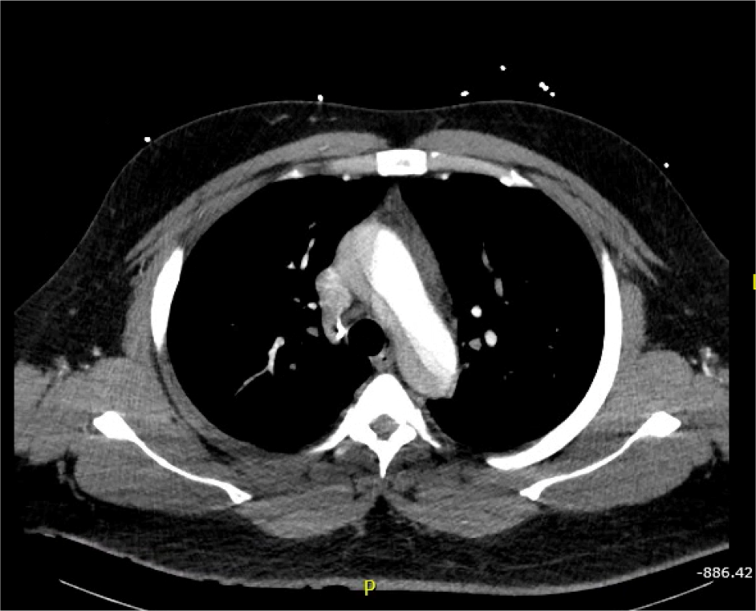
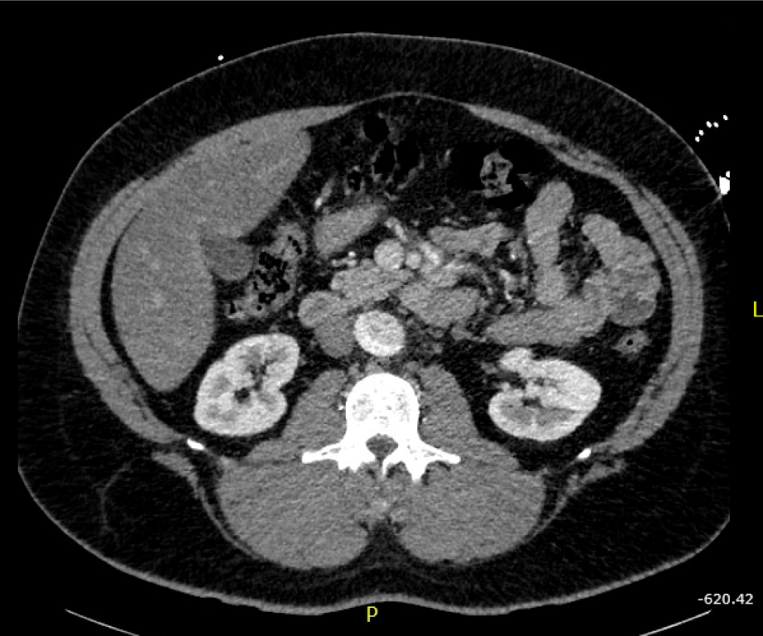
Patient’s initial EKG showed ST elevation in anterior leads, with possible ST depression in inferior leads, and T wave inversion in lateral leads. Given the patient’s clinical presentation and appearance, there was concern for ongoing ischemia. Based on the patient’s history of pain radiating into the abdomen and severe hypertension, there was additional concern for aortic dissection. This led to the cancelation of the catheterization lab activation. Slices of his computed tomography (CT) scan are shown below, revealing a severe type A aortic dissection, dissecting from the coronary arteries to the bilateral iliac arteries. Patient was started on nitroprusside and esmolol infusion and transferred emergently for cardiovascular surgery. He was discharged from the hospital in good condition less than one week later following an uncomplicated post-operative course.

Discussion
Cases of type A aortic dissection (TAAD) presenting as STEMIs are a well-documented, yet rare phenomenon, that are often missed in the emergency department. One study by Luo et al found increased mortality for patients with TAAD manifesting as acute myocardial infarction (AMI): 17% overall mortality for TAAD compared to 36% mortality in those manifesting as AMI.[1] This difference in mortality may be secondary to cardiac injury or related to the delay in care that comes from delay in diagnosis. In this study, a total of 5% of TAAD patients presented as AMI and all of them were diagnosed by coronary angiography (CAG). Another study, Zhu et al., found that STEMI secondary to TAAD occurred in only 0.5% of patients.[2] Five of these patients underwent coronary angiography without knowledge of the TAAD, with three of the five surviving. Another two patients received thrombolytic therapy prior to CAG and subsequently died. The authors reported an overall in-hospital mortality of 37.5% in this subset of patients, compared to a baseline mortality of TAAD patients of approximately 20%.[2,3]
Patients with concurrent TAAD and AMI have worse outcomes and increased mortality when compared to those with only TAAD. It is therefore important for emergency physicians to recognize when acute coronary syndrome may be secondary to an aortic dissection. Clues may include a description of pain, severe hypertension, or history of vascular disorders. Early recognition prior to heparinization and CAG will lead to earlier surgical intervention and thus improved patient outcomes.
References:
1. Luo JL, Wu CK, Lin YH, et al. Type A aortic dissection manifesting as acute myocardial infarction: still a lesson to learn. Acta Cardiol. 2009;64(4):499-504.
2. Zhu QY, Tai S, Tang L, et al. STEMI could be the primary presentation of acute aortic dissection. Am J Emerg Med. 2017;35(11):1713-1717.
3. Manning W, Black J. Overview of aortic syndromes. Up to date. 2017. Accessed on 6 Feb 2018. Available from: https://www.uptodate.com/contents/overview-of-acute-aortic-syndromes?search=type%20a%20aortic%20dissection&source=search_result&selectedTitle=3~150&usage_type=default&display_rank=3.