
 |
| This post was peer reviewed. Click to learn more. |
 |
| Image Credit: MaxPixel |
Authors: Justin Rafael De la Fuente, MSII
Medical Student
University of Miami Miller School of Medicine
Tim Montrief, MD MPH
Emergency Medicine Resident Physician
Jackson Memorial Health System
AAEM/RSA Publications & Social Media Committee
Jeffrey M Scott, DO
Attending Physician
Jackson Memorial Health System
Case
A 63-year-old man is brought in to the emergency department by ambulance after being found unresponsive at home by his family. He was last seen normal about four hours prior to arrival. En route, the patient was exhibiting irregular respirations with an oxygen saturation of 85% and was intubated by paramedics. On arrival, he is unresponsive with an oxygen saturation of 92%, bradycardic at 55 beats per minute, and hypertensive with a blood pressure of 160/95 mmHg.
The Comatose Patient: GCS vs. the FOUR Score
Comatose patients are defined as unresponsive with eyes closed and dysfunctional awareness. This presentation, combined with the large differential diagnosis involved, can make it challenging to evaluate a patient’s neurologic condition.[1] Emergency Neurological Life Support protocols developed by the Neurocritical Care Society recommend a focused neurologic exam that should include either the Glasgow Coma Scale (GCS), or a newer scale called the Full Outline Unresponsiveness (FOUR) Score, to assess level of consciousness.[2]
Currently, the GCS is widely used and is based on patient motor response, verbal response, and eye opening. However, it has several limitations for evaluating the comatose patient. For example, these patients often require intubation, leaving the emergency provider unable to assess verbal response.[3] Additionally, the GCS excludes evaluation of the brainstem and breathing patterns, important indicators of coma severity.[4] The GCS also has important drawbacks when used in the emergency department (ED). Studies have demonstrated poor inter-rater reliability among emergency physicians at all training levels, nurses, and pre-hospital staff.[5, 6] In the trauma setting, total GCS alone has been shown to have limited value, with mortality varying widely depending on the combination of component scores.[7] Finally, when asked to assess the GCS in standardized vignettes, a study of over 200 emergency providers demonstrated only 33.1% accuracy, calling into question its validity when utilized in the ED, especially by those inexperienced in its use.[8] The FOUR score accounts for many of these limitations, giving it an advantage in neurological assessment of the comatose patient over the GCS.
The FOUR score is broken into four components based on eye response, motor response, brainstem reflexes, and respiration. By including evaluation of breathing and the brainstem, the FOUR score provides more insight into coma severity. For example, the loss of brainstem reflexes may clue the provider in to a structural cause of coma. Within the literature, it has been shown that patients with the lowest FOUR score have substantially higher mortality than those with the lowest GCS.[4, 9] The eye response section of the FOUR score provides more information than that of the GCS by looking at eye tracking as opposed to eye opening, allowing the provider to assess for locked-in syndrome or a persistent vegetative state.[4] Importantly, the FOUR score does not require a verbal response in order to be calculated, meaning it can be properly applied in an intubated patient, unlike the GCS.
Utilizing the FOUR Score
Each component of the FOUR score is graded on a scale from 0 to 4. When testing eye response, a patient gets 4 points if able to blink or track on command, even if their eyelids must be opened by the examiner. They get 3 if the eyelids open but are unable to track, 2 if the eyelids are closed but open to loud voice, 1 if closed but open to pain, and 0 if they remain closed with pain.
In the motor response category, a patient receives 4 points if able to make a thumbs-up, fist, or peace sign, a test that has been validated as a reliable way to assess alertness.[10] Localizing to a painful stimulus earns 3, flexion response earns 2, an extension response earns 1, and a lack of response or a generalized myoclonus state receives 0.
When evaluating brainstem reflexes, the patient scores 4 points if pupil and corneal reflexes are present, 3 if one pupil is wide and fixed, 2 if pupil or corneal reflexes are absent, 1 if both of those reflexes are absent, and 0 if both of those reflexes are absent with an absent cough reflex.
The patient’s respiration score is 4 if they exhibit a regular breathing pattern and are not intubated, 3 if they are not intubated but exhibit Cheyne-Stokes breathing, 2 if they are not intubated and exhibiting irregular breathing, 1 if they are intubated but breathing above ventilator rate, and 0 if they are intubated and breathe at ventilator rate or are apneic (Table 1).
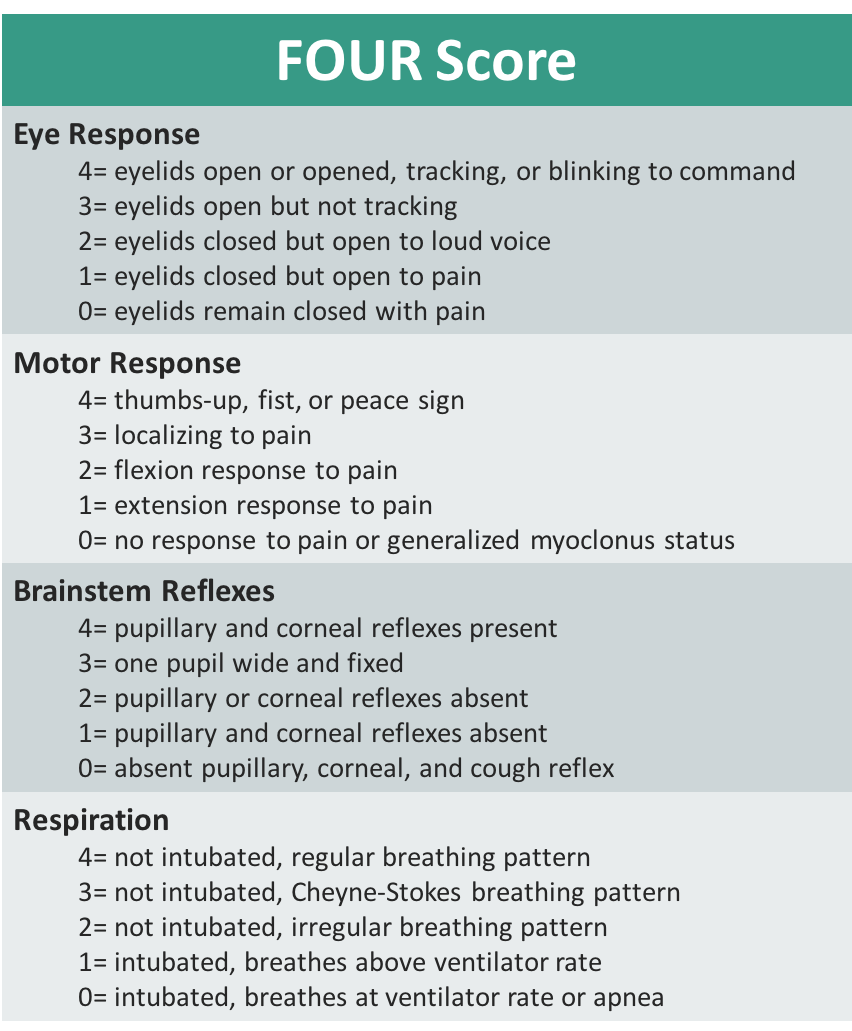 |
| Table 1: FOUR Score |
Evidence for the FOUR Score
Since its development, the FOUR score has been tested and validated in a number of studies and has shown to have good inter-rater reliability compared to the GCS.[4, 9, 11-14] It was first developed for use in the neurointensive care unit but has since been utilized in the medical intensive care unit and the ED. Furthermore, it has been validated by a variety of physicians at all levels of training, including those with and without a neurology background. These studie
s have also included nurses, and each time have maintained good inter-rater reliability.[4, 9, 12] The FOUR score is ready for more widespread use, and in certain situations such as the comatose patient, can be more useful than the GCS in neurologic assessment.
Case Conclusion
The patient’s condition and intubation prior to arrival precluded proper calculation of his GCS due to an inability to assess his verbal response. However, the FOUR score served to be a useful tool in his initial assessment. He had a score of E1, M2, B1, and R0, and because of the low scoring of brainstem reflexes, there was concern for a brainstem insult. After a non-contrast computed tomography (CT) of the head was read as negative for acute intracranial hemorrhage, interventional neuroradiology was consulted. CT angiography of the head was ordered, revealing a basilar artery stroke. His care was quickly transferred to the neuroradiology team for timely intervention.
References:
1. Orman R, Chang W. Coma. Emergency Medicine: Reviews and Perspectives. April 2017. Volume 17 Issue 4.
2. Cadena R, Sarwal A. Coma. Emergency Neurological Life Support. Available at: http://enlsprotocols.org:8080/protocols/enls-body.html?id=8##. Accessed September 15, 2018.
3. Teasdale G, Maas A, Lecky F, Manley G, Stocchetti N, Murray G. The Glasgow Coma Scale at 40 years: standing the test of time. Lancet Neurol. 2014;13(8):844-54.
4. Wijdicks EF, Bamlet WR, Maramattom BV, Manno EM, Mcclelland RL. Validation of a new coma scale: The FOUR score. Ann Neurol. 2005;58(4):585-93.
5. Gill MR, Reiley DG, Green SM. Interrater reliability of Glasgow Coma Scale scores in the emergency department. Ann Emerg Med. 2004;43(2):215-23.
6. Holdgate A, Ching N, Angonese L. Variability in agreement between physicians and nurses when measuring the Glasgow Coma Scale in the emergency department limits its clinical usefulness. Emerg Med Australas. 2006;18(4):379-84.
7. Healey C, Osler TM, Rogers FB, et al. Improving the Glasgow Coma Scale score: motor score alone is a better predictor. J Trauma. 2003;54(4):671-8.
8. Bledsoe BE, Casey MJ, Feldman J, et al. Glasgow Coma Scale Scoring is Often Inaccurate. Prehosp Disaster Med. 2015;30(1):46-53.
9. Iyer VN, Mandrekar JN, Danielson RD, Zubkov AY, Elmer JL, Wijdicks EF. Validity of the FOUR score coma scale in the medical intensive care unit. Mayo Clin Proc. 2009;84(8):694-701.
10. Wijdicks EF, Kokmen E, O’Brien PC. Measurement of impaired consciousness in the neurological intensive care unit: a new test. Journal of Neurology, Neurosurgery & Psychiatry 1998;64:117-119.
11. Bruno MA, Ledoux D, Lambermont B, et al. Comparison of the Full Outline of UnResponsiveness and Glasgow Liege Scale/Glasgow Coma Scale in an intensive care unit population. Neurocrit Care. 2011;15(3):447-53.
12. Stead LG, Wijdicks EF, Bhagra A, et al. Validation of a new coma scale, the FOUR score, in the emergency department. Neurocrit Care. 2009;10(1):50-4.
13. Wolf CA, Wijdicks EF, Bamlet WR, Mcclelland RL. Further validation of the FOUR score coma scale by intensive care nurses. Mayo Clin Proc. 2007;82(4):435-8.
14. Fischer M, Rüegg S, Czaplinski A, et al. Inter-rater reliability of the Full Outline of UnResponsiveness score and the Glasgow Coma Scale in critically ill patients: a prospective observational study. Crit Care. 2010;14(2):R64.