
 |
| Image Credit: Flickr |
Originally Published: Common Sense, March/April 2016
Author: Gregory K. Wanner, DO, PA-C
Thomas Jefferson University
Author: Andrew W. Phillips, MD, Med
Stanford University, Division of Critical Care
Read part 2 here: Improving Efficiency for Residents
Residency is a time for improvement. Improving procedural skills, gaining clinical acumen, and growing knowledge are chief goals during residency. Efficiency is also a necessary skill for the budding emergency physician. After learning the core knowledge of emergency medicine and becoming competent in procedures, efficiency is the next item for residents to emphasize. How can efficiency be improved? How can residents tell if they’re moving too slowly or too quickly? How can a resident improve efficiency without missing important details or skimping on documentation? We will answer these questions in a two-part series. In this first article, we will review the average patient volume seen by residents, the concept of relative value units (RVUs), and touch on the idea of efficiency. In part two, in the next issue of Common Sense, we will discuss methods for improving efficiency based on expert recommendations and research.
Patients Per Hour
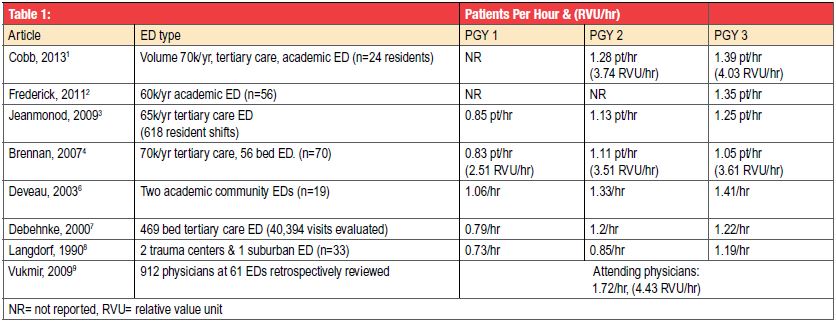
Residents often ask, “How many patients should I see per hour?” The answer is complicated. A resident’s patients per hour (pts/hr) rate depends upon many factors. Table 1 provides a general idea about the average number of pts/hr seen by residents. Several studies indicate that the pts/hr increases from intern year to senior year. However there is some overlap between each year of training. Across all included studies, interns (PGY1) averaged from 0.73 to 1.06 pts/hr; PGY2 residents ranged from 0.85 to 1.33; and senior (PGY3) residents ranged from 1.05 to 1.41.[1-8] Administrative and supervisory responsibilities also increased for senior residents, perhaps reducing the number of pts/hr for PGY3 residents to some degree.[3-4] As a comparison, two studies evaluated patients seen per hour by attendings. A retrospective study of 912 attending physicians at 61 EDs showed an overall average of 1.72 (SD=+/- 0.44) pts/hr, with physicians at higher volume (over 45,000 visits/year) EDs seeing 2.07 (SD=+/- 0.32) pts/hr.[9] Another study of attending physicians indicated an average of 1.87 pts/hr while working alone and 1.99 pts/hr while working with residents.[10] Bear in mind that this is at academic centers — by definition, since we’re discussing residents. Moreover, the numbers reflect not only physician speed but also patient demographics, such as whether or not pediatric patients are included or if there is a Fast Track that siphons away less complex patients – factors which are generalized in our summary.
Factors Affecting Efficiency
Several factors affect how many patients a resident sees per hour, including shift length, patient acuity, procedures, distractions, number of consecutive shifts, and the resident’s level of training.[3-5,11,12] Many of these factors change on a regular basis. Other dynamics, such as patient boarding and the number of sign-outs, also likely influence the number of patients seen per hour. Interestingly, neither ED volume changes nor working with medical students appears to have a significant effect on patients seen per hour by residents.[1,3] Length of shifts and number of consecutive shifts can influence the volume of patients seen per hour. Longer shifts appear to reduce productivity, as reported in a study of PGY-2 residents who saw 1.15 pts/hr during 9-hour shifts and 1.06 pts/hr during 12-hour shifts.[5] Conversely, productivity appears to increase with each consecutive shift. One study showed all levels of residents increased their average number of pts/hr over three consecutive shifts. For example, PGY3 resident pts/hr increased from 1.19 to 1.24 to 1.33 over three shifts.[11] Distractions, however, can reduce productivity. Emergency physicians are interrupted an average of every 5.8 minutes and are required to unexpectedly switch tasks every 8.7 minutes. The number of distractions increases with each additional patient being managed simultaneously.[12] These factors should be considered when trying to increase clinical efficiency.
The Value of Efficiency
Becoming more efficient in the ED will benefit your patients and will eventually be financially beneficial to you. Resident compensation is not based on productivity, but that changes for many attendings. Increased efficiency will typically lead to higher pay as an attending. Many attending jobs base compensation – either a portion or sometimes all – on productivity, often quantified by the relative value unit (RVU). The RVU is a calculation based on physician work, practice expenses, and malpractice insurance costs.[9,13] Using RVUs to estimate productivity is likely more accurate than simply looking at the number of patients seen per hour. Table 1 reviews two resident studies and one attending study reporting RVU values.[1,4,9] Both resident studies show an increase in RVUs for each year of training. One study reveals an increase in RVUs for PGY-3 residents despite a decrease in the number of patients seen per hour, compared to PGY-2 residents.[4]
Increasing Efficiency
With so many uncontrollable factors, the natural question to ask is how to improve the factors that are within your control. Fair warning: there is little research and a lot of expert opinion, but the advice is theoretically quite sound. In the next issue we will share advice from experts and research findings on how to improve your efficiency — safely.
 |
| TABLE 1 Click to enlarge. |
1. Cobb T, Jeanmonod D, Jeanmonod R. The impact of working with medical students on resident productivity in the emergency department. West J Emerg Med. 2013;14(6):585-9. PMID: 24381676
2. Frederick RC, Hafner JW, Schaefer TJ, Aldag JC. Outcome measures for emergency medicine residency graduates: do measures of academic and clinical performance during residency training correlate with American Board of Emergency Medicine test performance? Acad Emerg Med. 2011;18 Suppl 2:S59-64. PMID: 21999560
3. Jeanmonod R, Brook C, Winther M, Pathak S, Boyd M. Resident productivity as a function of emergency department volume, shift time of day, and cumulative time in the emergency department. Am J Emerg Med. 2009;27(3):313-9. PMID: 19328376
4. Brennan DF, Silvestri S, Sun JY, Papa L. Progression of emergency medicine resident productivity. Acad Emerg Med. 2007;14(9):790-4. PMID: 17726123
5. Jeanmonod R, Jeanmonod D, Ngiam R. Resident productivity: does shift length matter? Am J Emerg Med. 2008;26(7):789-91. PMID: 18774044
6. Deveau JP, Lorenz JE, Hughes MJ. Emergency medicine resident work productivity and procedural accomplishment. J Am Osteopath Assoc. 2003;103(6):291-6. PMID: 12834102
7. Debehnke D, O’brien S, Leschke R. Emergency medicine resident work productivity in an academic emergency department. Acad Emerg Med. 2000;7(1):90-2. PMID: 10894249
8. Langdorf MI, Strange G, Macneil P. Computerized tracking of emergency medicine resident clinical experience. Ann Emerg Med. 1990;19(7):764-73. PMID: 2389860
9. Vukmir RB, Howell RN. Emergency medicine provider efficiency: the learning curve, equilibration and point of diminishing returns. Emerg Med J. 2010;27(12):916-20. PMID: 21076164
10. Bhat R, Dubin J, Maloy K. Impact of learners on emergency medicine attending physician productivity. West J Emerg Med. 2014;15(1):41-4. PMID: 24578767
11. Jeanmonod R, Damewood S, Brook C. Resident productivity: trends over consecutive shifts. Int J Emerg Med. 2009;2(2):107-10. PMID: 20157452
12. Chisholm CD, Collison EK, Nelson DR, Cordell WH. Emergency department workplace interruptions: are emergency physicians “interrupt-driven” and “multitasking”? Acad Emerg Med. 2000;7(11):1239-43. PMID: 11073472
Medicare Physician Fee Schedule. Department of Health and Human Services. December 2014. https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNProducts/downloads/medcrephysfeeschedfctsht.pdf