
{kind=link}
 |
| Image Credit: Piqsels |
 |
| This post was peer reviewed. Click to learn more. |
PGY-1, Orthopedic Surgery
Additional Authors:
PGY-1, Orthopedic Surgery
PGY-1, Emergency Medicine
Naval Medical Center San Diego
AAEM/RSA Publications and Social Media Committee
Lightning strikes occur commonly, with an estimated global incidence of 240,000 worldwide per year with deaths numbering 24,000.[1] As more people embark on expeditions and explore the outdoors, they are putting themselves at risk of these strikes. Due to the prevalence and mortality of lightning strikes, emergency medicine physicians and other healthcare providers should be adept in treating these life-threatening injuries. This article reviews the guidelines for triage and management of cardiac emergencies due to lightning.
The Wilderness Medical Society (WMS) guidelines for the treatment and prevention of lightning injuries were first developed in 2011, and then updated in 2014 when experts in the field reviewed the current literature and created recommendations based on those results. The WMS has now incorporated classification guidelines from the American College of Chest Physicians in their updated guidelines. This paper highlights information relevant to practitioners in the emergency department.
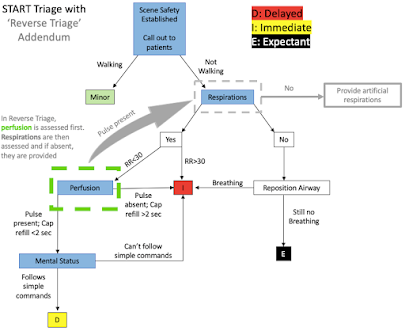 |
| ‘Reverse Triage’ Addendum |
Reverse Triage
Lightning strikes cause cardiac and respiratory arrest due to the depolarization of all myocardial cells.[2] Although asystole and ventricular fibrillation are the two most common abnormal rhythms observed after strikes, patients can regain return of spontaneous circulation (ROSC) due to the heart’s physiologic automaticity.[3] Once this occurs, the medullary respiratory center may spontaneously return the respiratory drive; however, if respiratory function is not regained then the patient can go into ventricular fibrillation and suffer a second cardiac arrest.[3] Nevertheless, if patients survive the initial lightning strike then they have a high chance of living.[4]
Lightning strikes often hit more than one person, as people will often walk in proximity, leading to mass casualty scenarios.[2] In a typical mass casualty scenario, the START triage dictates that patients not spontaneously breathing have their airway repositioned and if there is still not spontaneous breathing, then they be labeled expectant.[5] As mentioned above, because ROSC precedes the return of autonomous respiratory system function, it is vital to first provide ventilation to those who have a pulse. Thus, patients that are not spontaneously breathing ought to be treated, and “reverse triage” must be implemented when faced with a mass casualty scenario due to lightning strikes.[3] With this system, priority is placed on treating those with no spontaneous respirations, because in this scenario, they have a higher potential for recovery than the original START algorithm implies.
Resuscitation
After being struck, it is safe to triage and resuscitate casualties immediately. The WMS recommends initiating basic and advanced life support algorithms immediately as indicated, in addition to managing trauma.[6,7] With direct strikes, it is more common to see sudden death or severe electrocardiogram (EKG) changes, whereas contact strikes or ground current (indirect contact with lightning strike) may only produce transient EKG changes. These EKG changes include ST segment elevation, prolonged QT interval, and atrial fibrillation, and labs can show elevated cardiac markers. Additionally, there are reports of delayed EKG changes following a lightning strike, with reports of EKG changes three days after the event.[8]
For patients suffering from a direct strike or complaining of chest pain or dyspnea, they should receive an EKG and echocardiogram. In the absence of other obvious injuries, cardiac dysrhythmia should be ruled out if the patient is in shock. If any changes are found or if the patient suffered a direct strike, it is recommended the patient be admitted to the hospital for monitoring via telemetry for at least 24 hours to determine if the changes are reversible.[2] Remember to note their previous cardiac history as well as other chronic conditions, which may be exacerbated by this acute strike. The WMS describes that elevated cardiac markers such as elevated troponins are non-prognostic of coronary artery disease complications and have limited clinical utility in this context, because they may not correlate with a chronic coronary artery disease but rather an acute electrophysiologic insult.[8,9] If the patient is safe for discharge, they should be instructed to return if they develop chest pain or dyspnea because these could be signs of delayed cardiomyopathy or pericarditis.[2]
Discussion
The guidelines listed above are recommendations from the Wilderness Medical Society based on the review of numerous case reports and based on expert advice. When faced with a patient who suffered a lightning strike, emergency medicine residents and medical students can use these recommendations to guide their treatment. The most crucial point to follow is to perform reverse triage immediately following a lightning strike to help the greatest number of people and to start cardiopulmonary resuscitation as soon as possible. Once in the emergency department, ECG and echocardiogram should guide further treatment.
References:
1. Ronald L. Holle. Annual rates of lightning fatalities by country. 20th International Lightning Detection Conference. 2008.
2. Davis C, Engeln A, Johnson EL, et al. Wilderness Medical Society practice guidelines for the prevention and treatment of lightning injuries: 2014 update. Wilderness Environ Med. 2014;25(4 Suppl):S86-95. doi: 10.1016/j.wem.2014.08.011
3. Taussig HB. “Death” from lightning and the possibility of living again. Am Sci. 1969;57(3):306-16.
4. Cooper MA. Lightning injuries: prognostic signs for death. Ann Emerg Med. 1980;9(3):134-8. doi: 10.1016/s0196-0644(80)80268-x
5. Benson M, Koenig KL, Schultz CH. Disaster triage: START, then SAVE-a new method of dynamic triage for victims of a catastrophic earthquake. Prehospital Disaster Med. 1996; Apr-Jun; 11(2): 117-24. doi: 10.1017/s1049023x0004276x
6. ECC Committee, Subcommittes and Task Forces of the American Heart Association. 2005 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2005;112(24 Suppl):IV1-203. doi: 10.1161/CIRCULATIONAHA.105.166550
7. Driscoll P, Wardrope J. ATLS: past, present, and future. Emerg Med J. 2005;22(1):2-3. doi: 10.1136/emj.2004.021212
8. Lichtenberg R, Dries D, Ward K, Marshall W, Scanlon P. Cardiovascular effects of lightning strikes. J Am Coll Cardiol. 1993;21(2):531-6. doi: 10.1016/0735-1097 (93)90699-2
9. Saglam H, Yavuz Y, Yurumez Y, Ozkececi G, Kilit C. A case of acute myocardial infarction due to indirect lightning strike. J Electrocardiol. 2007;40(6):527-30. doi: 10.1016/j.electrocard.2007.03.015