
 |
| Image Credit: Pexels |
 |
| This post was peer reviewed. Click to learn more. |
Authors: Grant Barker, MS4
University of Miami Miller School of Medicine
Tim Montrief, MD MPH
Jackson Memorial Health System/University of Miami
AAEM/RSA Publications and Social Media Committee Member
Case
While spearfishing for lionfish off the coast of Key West during one of our yearly excursions, my father was unfortunate enough to graze a lionfish’s spines with his thumb. Within the next ten minutes, he was hyperventilating and in extreme pain. On our small boat with just a rudimentary first aid kit, thirty miles from shore, we had minimal interventions at our disposal. What would your next step in treatment?
Introduction
The American Association of Poison Control Centers’ National Poison Data System reported 724 single exposures for fish, jellyfish, and other coelenterate (such as anemone) stings in 2016.[1] This likely underestimates the number of exposures, as the data only accounts for those envenomations reported to poison control centers. It is important to understand the relatively simple therapies that underlie appropriate care for these unusually painful and potentially morbid injuries. The treatments for several different evenomations have many similarities, with a focus on analgesia, supportive care, and wound management (Figure 1).
Vertebrates
- Scorpaenidae
Scorpaenidae are a family of marine fish with venomous spines that includes lionfish, scorpionfish, and stonefish. Lionfish are the least venomous of the three, but account for the most envenomations. Lionfish are native to the Indo-Pacific region, but are commonly kept as aquarium fish. They are also an invasive species that has established itself on the East Coast of the United States and Caribbean. Scorpionfish are commonly found along the California coast. Stonefish are native to the Indo-Pacific region, and are one of the most venomous fish in the world, with a neurotoxin that acts on both skeletal and smooth muscle.
Systemic effects of Scorpaenidae envenomation are rare, but may include headache, vomiting, abdominal pain, delirium, seizures, limb paralysis, hypo- or hypertension, respiratory distress, arrhythmias, and congestive heart failure. One account reported pulmonary edema from a stonefish sting beginning just 35 minutes after injury.[2] Local effects include edema, erythema, and severe pain. The pain peaks around 60 minutes and often resolves in 6-12 hours.
Treatment for Scorpaenidae envenomation centers around infection control and analgesia. It is also important to consider possible systemic effects of toxin, especially in the case of stonefish. There is a stonefish antivenin available that can be located through regional poison control centers.
Hot water immersion (105°-115°F) as tolerated for 30-90 minutes is the first step to achieving adequate pain control, as it degrades the venom’s heat-labile proteins. Additionally, a strategy incorporating oral or parenteral analgesics, as well as local anesthetics, is appropriate.
All wounds should be irrigated and explored, spines should be removed, and necrotic tissue debrided. Prophylactic antibiotics are recommended for wounds with high risk of infection including those with suspected foreign body, contaminated or deep wounds, and wounds in immunocompromised patients. Antibiotics should cover standard gram-positive skin flora as well as Vibrio and Aeromonas, both common microbes in saltwater exposures.[3] Vibrio can be covered with a combination of docycycline 100mg twice daily and ceftriaxone 1g, or levofloxacin 750mg once daily. Tetanus vaccination status and need for prophylaxis should also be assessed. Finally, patients should be observed for four hours to ensure systemic symptoms and adequate analgesic control. Systemic symptoms or refractory pain should prompt consideration for inpatient admission.
- Stingrays
Stingray envenomations are typically the result of a defensive reflex: whipping the barbed tail forward when the wings of the ray are touched. Achieving hemostasis is imperative, followed by analgesic control through hot water immersion for thirty minutes before attempting to remove the barb. Wounds penetrating the chest, neck, or peritoneal cavity require exploration in the operating room and should be managed in a similar manner to a penetrating trauma. For other wounds, care and analgesic recommendations are the same as for Scorpaenidae above.
Invertebrates
- Cnidaria
Phylum Cnidaria includes hydroids, fire coral, jellyfish, and anemones. The phylum name refers to an organelle called a cnida (more commonly known as a nematocyst), which contains a coiled hollow tubule with a barb attached. The external side of the cnida has a trigger called a cnidocil, which is both a mechano- and chemoreceptor. When this trigger is activated, the cnida discharges the barb and delivers the toxic content.
Reactions to stings may be localized or systemic. While anaphylaxis is rare, mild allergic reactions, including erythema nodosum, are not uncommon.[4] Stings generally cause an acute, painful, dermatitis that resolves spontaneously in hours to days after the exposure. Larval forms of jellyfish and anemones may cause an intensely pruritic hypersensitivity reaction known as “seabather’s eruption,” which typically begins after one takes a shower after the exposure.
Cnidaria stings are treated by soaking the affected area in 5% acetic acid (household vinegar). Freshwater and abrasion of the wound should be avoided as these may cause additional nematocyst firing. Remaining nematocysts may be removed by shaving the area. Following primary decontamination, topical corticosteroids such as hydrocortisone 2% and oral antihistamines can be used to treat excessive pruritus and dermatitis.
Two notable exceptions are the box jellyfish and the Irukandji jellyfish, found in the Indo-Pacific. The box jellyfish is colloquially known as the most venomous marine animal on earth, causing death through rapid hypotension and cardiovascular collapse. An antivenin is available through regional poison centers, and one 20,000 unit vial intravenous (IV) should be the initial therapy in cases of cardiogenic shock or cardiac arrest. Conversely, stings from the Irukandji jellyfish are known to trigger catecholamine release, causing severe hypertension and occasionally intracerebral hemorrhage.[5] Treatment of Irukandji stings is mainly supportive.
- Sea Urchins
Sea urchins may cause injury through local venom toxicity as well as penetrating injury. Skin penetration by more than 15-20 spines puts the patient at risk of systemic toxicity characterized by paresthesias, muscular paralysis, hypotension, and respiratory distress.[6]
Oral analgesia and hot water immersion are the basis of treatment for urchins. X-ray or ultrasound should be utilized to evaluate for retained spines, which are made of calcium carbonate and are radiopaque. These can result in severe synovitis if in a joint, or lead to infection or granuloma formation.[7] It is important to note that purple dye may leach from spines and be mistaken for a retained spine.
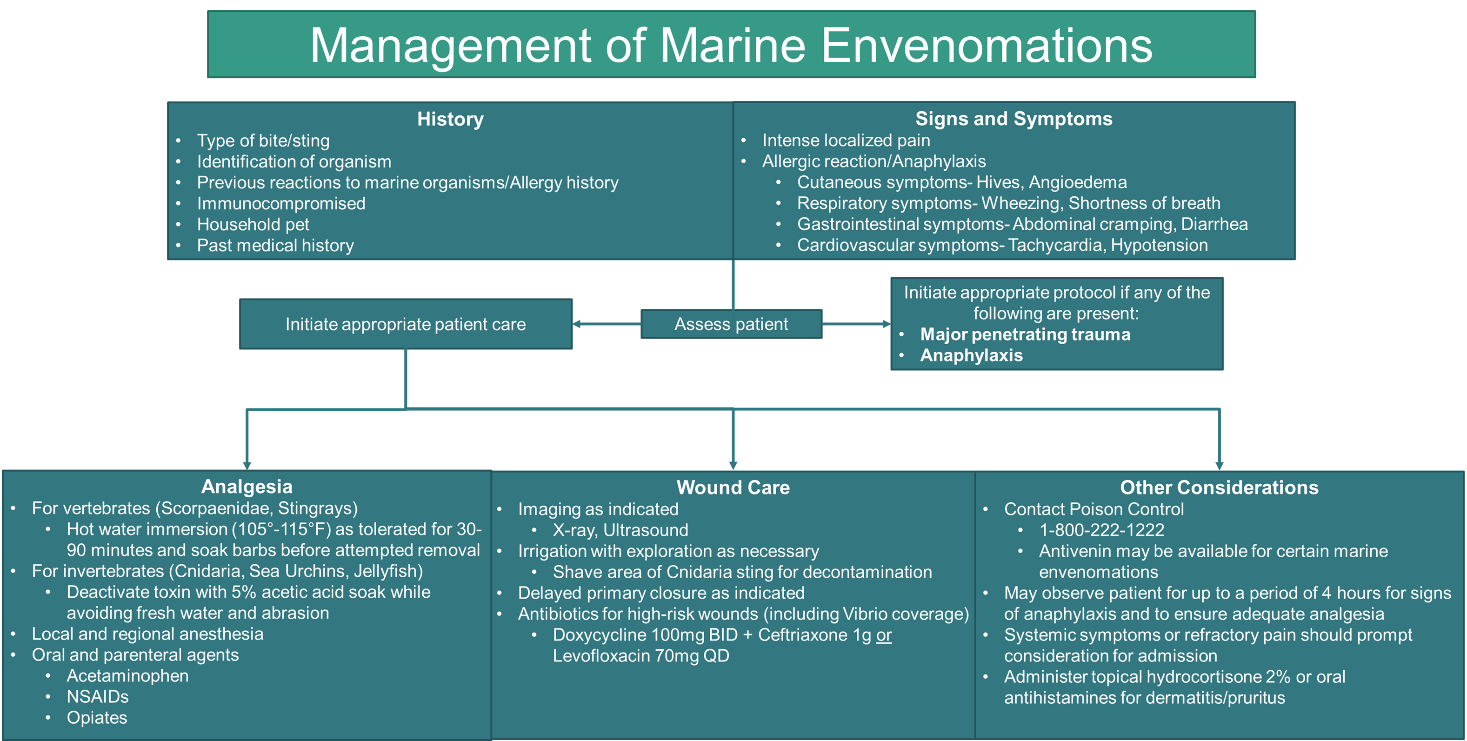 |
| Figure 1. Management of marine envenomation algorithm |
The Undifferentiated Envenomation
For the patient who doesn’t know what they were stung by, considering the type of marine environment may help elucidate the species. Scorpaenidae is typically a reef-dwelling fish that catches prey by ambush. As such, this would be unlikely in a patient who was envenomated while walking in shallow surf. It is important that the prudent clinician know their local dangerous marine fauna as well, and most regional poison control centers and state departments of health have this data available. If there is a possibility of life-threatening fauna such as the box jellyfish or the presence of systemic symptoms, poison control should be contacted (1-800-222-1222). In absence of previous reaction or allergy history, the above algorithm can be followed in regards to analgesia, wound care, and disposition.
Case Conclusion
My father, the knowledgeable emergency physician that he is, put his thumb in my perfectly good thermos of hot coffee, while explaining that it is a heat-labile venom. Within minutes the pain subsided. While he nursed his thumb, I drove the boat in to get more hot water.
References:
1. Gummin DD, Mowry JB, Spyker DA, Brooks DE, Fraser MO, Banner W. 2016 Annual Report of the American Association of Poison Control Centers’ National Poison Data System (NPDS): 34th Annual Report. Clin Toxicol (Phila) 2017;55:1072–1252.
2. Lehmann DF, Hardy JC. Stonefish envenomation. N Engl J Med. 1993;329(7):510-1.
3. Auerbach PS. National Lecture Series: Hazardous Marine Envenomations. Emergency Medicine: Reviews and Perspectives 2017; 17(10).
4. Togias A.G., Burnett J.W., Kagey-Sobotka A., Lichtenstein L.M. Anaphylaxis after contact with a jellyfish. J. Allergy Clin. Immunol. 1985;75:672–675. doi: 10.1016/0091-6749(85)90092-2.
5. Fenner P. Marine envenomations: an update—a presentation on the current status of marine envenomations first aid and medical treatments. Emerg Med Aust 2000;12:295-302.
6. Auerbach PS. Marine envenomations. N Engl J Med. 1991;325(7):486-93.
7. Balhara KS, Stolbach A. Marine envenomations. Emerg Med Clin North Am. 2014;32(1), 223-243. doi: 10.1016/j.emc.2013.09.009