

{kind=link}
Author: Fernando Pellerano, MS-4
Medical Student, Universidad Iberoamericana (UNIBE)
 |
| This post was peer reviewed. Click to learn more. |
Ocular emergencies are immediate threats to the visual system that can lead to permanent loss of visual function.[1] Emergency medicine physicians should be able to recognize and provide initial treatment for sight-threatening ophthalmologic emergencies, including globe injury, before referral to an ophthalmologist.
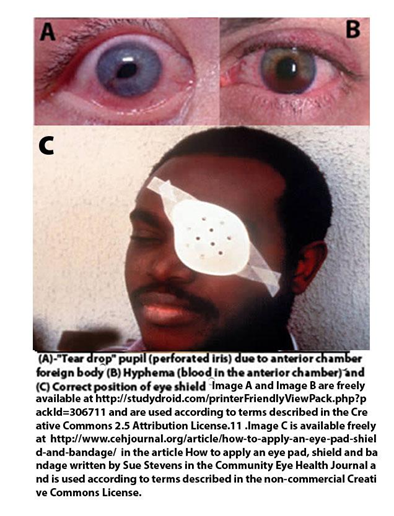
Globe rupture should always be considered as a differential diagnosis in a patient with an eye injury. Patients will complain of moderate to severe pain and decreased vision. Visual acuity may be limited to “counting fingers at 18 inches” or “light perception only.” Pupils should be examined for shape, size, light reflex, and afferent pupillary defect. A peaked, teardrop-shaped, or otherwise irregular pupil may indicate globe rupture (see Image A).[2] Hyphema (blood in the anterior chamber: see Image B) or severe conjunctival hemorrhage involving the area around the cornea are also highly suspicious for globe injury.[2] Physicians may perform the Siedel’s Test to detect aqueous humor leaking from a corneal wound. To perform the test, a fluorescein dye is applied to the affected eye and examined under slit-lamp. The test is positive when a stream of fluorescent dye is seen emanating from the affected eye.[3]
In a penetrating globe injury, measurement of intraocular pressure is contraindicated to avoid applying pressure on the globe. If the intraocular pressure is measured the contents of the globe may extrude onto the cheek.[4] In young children where the extent of intraocular injury cannot be assessed because of poor cooperation, the physical exam can be performed under conscious sedation with the support of an ophthalmologist.[2]
After the appropriate history and physical exam the emergency medicine physician should follow these basic steps:
- Keep the patient NPO (not eating anything) in the event that surgery is required.
- Place an eye shield over the affected eye (see Image C), and obtain a computed tomography (CT) scan of the head and orbits (coronal and axial views) to evaluate for open globe injury, intraocular foreign body, and orbital wall fractures.[5] An orbital foreign body that may have perforated the globe should be left undisturbed until surgery. A rupture of the globe may present with enophthalmos (recession of the globe within the orbit) and orbital crepitus, an indication of subcutaneous emphysema potentially from an associated sinus fracture.[2]
- Document tetanus immune status and update as indicated. An open globe laceration is considered a tetanus prone wound.[5]
- Start systemic broad spectrum antibiotics within six hours of the injury. If not treated promptly and appropriately, the patient may develop endophthalmitis, a serious intraocular infection that can cause blindness. An acceptable antibiotic regimen for adults is intravenous vancomycin hydrochloride 1g every 12 hours, ceftazidime 2g every 12 hours, and ciprofloxacin 400mg every 12 hours. (Patients older than 60 years old, taking steroids, or those with a kidney, heart or lung transplant are at increased risk of tendon rupture after taking ciprofloxacin, and they should immediately consult their provider if they develop any tendon related pain).[9] Antibiotic treatment for children should include intravenous cefazolin 25 to 50mg per kg every 8 hours plus intravenous gentamicin 2mg per kg every 8 hours. [6]
- Administration of an antiemetic (e.g., prochlorperazine 10mg intravenous or ondansetron 8mg) and analgesia (e.g., morphine or hydromorphone) can be used to prevent any pressure on the globe that may lead to extrusion of the intraocular content.[5,7,8]
- Ophthalmology consultation and referral is mandatory, and the patient needs to be admitted or transferred. The involved eye is kept shielded with no patch, and the patient is put on bedrest until a definitive care plan is established.[7]
Overall, when talking about ocular emergencies the rapid diagnosis, treatment, and correct referral are the ultimate determinants of the patient’s ocular well-being and prognosis.
References
1. Khare, G.D., Symons, A., & Do, D.V. Common Ophthalmic Emergencies. International Journal of Clinical Practice 2008; 62(11), 1776-1784. Available from http://www.medscape.com/viewarticle/583742.
2. Acerra J, Drone S. Globe Rupture Clinical Presentation. Medscape. March 2014.available from http://emedicine.medscape.com/article/798223-clinical#a0217.Accessed October 23, 2014.
3. Nickson C. Eyes Wide Split. Life in the fastlane. 2011. Available from http://lifeinthefastlane.com/ophthalmology-befuddler-013/ . Accessed October 23, 2014.
4. Goldberg, S., & Trattler, W. Ophthalmology Made Ridiculously Simple. Miami, FL: MedMaster, Inc.; 2012.
5. Pokhrel, P., Loftus, S. Ocular Emergencies. Am Fam Physician. 2007; 76(6), 829-836. Available from http://www.aafp.org/afp/2007/0915/p829.html
6. Kuhn F, Pieramici D. Ocular Trauma Principles and Practice. In: Chaudhry N, Flynn H ed. Endophthalmitis. 1st ed. New York , NY: Thieme Medical Publishers, Inc; 2002:296.
7. Limkakeng A, Schaider J .Globe Rupture. In: Schaider J, Barkin R, Hayden S, Wolfe R, Barking A, Shayne P, Rosen P, ed. Rosen & Barkin’s 5-Minute Emergency Medicine Consult. 4th ed.USA: Lippincott Williams & Wilkins; 2010.
8. Palay D, Krachmer J. Palay & Krachmer: Primary Care Ophthalmology, 2nd ed. USA: Mosby, An imprint of Elsevier; 2005.
9. Information for Healthcare Professionals: Fluoroquinolone Antimicrobial Drugs [ciprofloxacin (marketed as Cipro and generic ciprofloxacin), ciprofloxacin extended-release (marketed as Cipro XR and Proquin XR), gemifloxacin (marketed as Factive), levofloxacin (marketed as Levaquin), moxifloxacin (marketed as Avelox), norfloxacin (marketed as Noroxin), and ofloxacin (marketed as Floxin)]. August 15, 2013. Available at: http://www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/ucm126085.htm. Accessed January 26, 2015.