
 |
| Image Credit: Pixabay |
Author: Jake Toy, MS3
Western University of Health Sciences, College of Osteopathic Medicine of the Pacific, Pomona, CA
AAEM/RSA Publications Committee ’16-’17
 |
| This post was peer reviewed. Click to learn more. |
Heart disease is the leading cause of morbidity and mortality among women in the United States and accounts for approximately 1 in 4 deaths among women.[1] Unfortunately, society fails to recognize this burden, often labeling heart disease as a “male problem”. In the past decade, only 54% of women recognized heart disease as a number 1 cause of mortality.[2] Exacerbating this issue further, the “classic” symptoms of myocardial infarction (MI) were historically based off studies analyzing MI in men.[3] Additionally, women often experience greater delays in care during an MI and have higher associated mortality rates when compared to men.[4, 5]
A significant body of literature exists describing sex-specific differences in MI presentation and outcomes. In the emergency department (ED), awareness of these variances in MI presentation is crucial toward providing timely and effective care to women presenting with an acute MI.
Typical vs. Atypical Chest Pain
The textbook symptoms of “typical” chest pain are well-defined – (1) precordial chest discomfort, pain, heaviness, or fullness, possibly radiating to the arm, shoulder, back, neck, jaw, or epigastrium; (2) symptoms worsened by stress or activity; (3) symptoms relieved by rest or medications, such as nitroglycerin; (4) associated symptoms that include shortness of breath, diaphoresis, weakness, nausea, vomiting, or lightheadedness.[3]
In comparison, “atypical” chest pain does not present in the aforementioned classic pattern. Signs may include: burning, sharp, pleuritic, or positional chest pain or discomfort; chest pain that is localized by one finger and reproducible; pain only in the arm, shoulder, back, neck, jaw, or epigastrium, or pain concentrated in regions of the body other than the chest, arm, shoulder, back, neck, jaw, or epigastrium.[3]
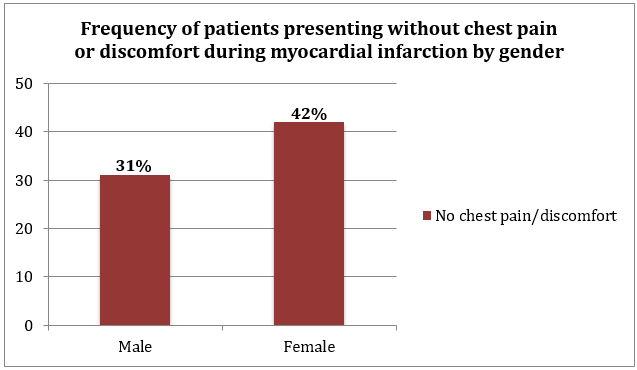
What percentage of women are likely to present to the ED with an atypical presentation?
Approximately 1 in 3 MI patients present without chest pain.[6] Among this proportion, women were more likely to present in this “atypical” fashion than men (42% vs. 30.7% respectively) and also tend to exhibit more non-specific acute symptoms than men.[6] Multiple studies have further noted a significant interaction between sex and age as predictors of the absence of chest pain in MI patients.[3, 6, 7] Younger females (<45 years old) may be 30% more likely to present without chest pain than similar aged males who present without chest pain; however, as age increases, this difference in presentation is attenuated.[6] However, other studies that stratified analyses by age group, noted that age was a stronger predictor of MI presentation without chest pain than sex.[3, 5]
Understanding these age and sex-specific differences in MI presentation are especially important because they likely contribute to the higher overall in-hospital mortality rate experienced by women in cases of MI in comparison to men (14.6% vs. 10.3% respectively).[6] Further, younger women with who did not report chest pain upon presenting with a MI have a significantly higher mortality rate in comparison to similar aged men who presented without chest pain.[6] This difference also appears to attenuate with age. These increased mortality rates may be explained by the fact that those MI patients who present without chest pain often have a delay in treatment by up to 2 hours.[5]
Conclusions
It is important to keep in mind that chest discomfort still remains the most commonly reported MI symptom in both men and women.[5] However, a significant portion of patients also present without chest pain, and in this proportion, mortality is significantly increased. Further, women make up a greater percentage of patients that present in this atypical fashion. As such, emergency clinicians must be cognizant of these sex-based differences, and have a high index of suspicion when a 45-year-old female patient with cardiac risk factors presents to the ED with a “lump in her throat” or “nausea and epigastric pain”. Missing an MI in these cases may prove fatal.
References
1. Xu J, Murphy SL, Kochanek KD, Bastian BA. Deaths: Final Data for 2013. Natl Vital Stat Rep. 2016 Feb 16;64(2):1-119.
2. Mosca L, Mochari-Greenberger H, Dolor RJ, Newby LK, Robb KJ. Twelve-year follow-up of American women’s awareness of cardiovascular disease risk and barriers to heart health. Circ Cardiovasc Qual Outcomes. 2010 Mar;3(2):120-7.
3. Canto JG, Goldberg RJ, Hand MM, et al. Symptom presentation of women with acute coronary syndromes: myth vs reality. Arch Intern Med. 2007 Dec 10;167(22):2405-13.
4. Yu J, Mehran R, Grinfeld L, et al. Sex-based differences in bleeding and long term adverse events after percutaneous coronary intervention for acute myocardial infarction: three year results from the HORIZONS-AMI trial. Catheter Cardiovasc Interv. 2015 Feb 15;85(3):359-68.
5. Canto JG, Shlipak MG, Rogers WJ, et al. Prevalence, clinical characteristics, and mortality among patients with myocardial infarction presenting without chest pain. JAMA. 2000 Jun 28;283(24):3223-9.
6. Canto JG, Rogers WJ, Goldberg RJ, et al. Association of age and sex with myocardial infarction symptom presentation and in-hospital mortality. JAMA. 2012 Feb 22;307(8):813-22.
7. Graham G. Acute Coronary Syndromes in Women: Recent Treatment Trends and Outcomes. Clin Med Insights Cardiol. 2016;10:1-10.