
 |
| Image Credit: Pixabay |
 |
| This post was peer reviewed. Click to learn more. |
Author: Nick Pettit, DO PhD
Resident Physician, Indiana University
AAEM/RSA At-Large Board Member
Malignancy is the second leading cause of mortality, and scarily, retrospective studies have demonstrated that the projected five-year survival once someone receives a diagnosis of cancer is approximately 50%. The National Cancer Institute recently expanded its research agenda to better understand cancer care in the ED. Studies have shown that cancer patients make up about 3% of emergency department (ED) visits and Medicare data has demonstrated that in the last six months of life, cancer patients utilize the ED significantly more.[1]
Cancer-related emergencies may result from mass effect from expanding malignancies (i.e. obstruction, superior vena cava syndrome, tamponade), infectious issues, or metabolic issues such as tumor lysis syndrome, hypercalcemia, or syndrome of inappropriate antidiuretic hormone secretion (SIADH). This article focuses on tumor lysis syndrome (TLS).
TLS is a rare but life-threatening metabolic disorder associated with malignancy. It often presents 6-72 hours after chemotherapy or radiation therapies, or occasionally as the presenting derangement due to rapidly proliferating tumors with significant growth (i.e. leukemias or lymphomas). Clinically these patients are tired, possibly lethargic, weak, nauseated and vomiting, crampy, or even in full blown cardiac arrest. Regarding laboratory values, once the tumor cells lyse, they release potassium and phosphorus, causing hyperkalemia and hyperphosphatemia. This phosphorus binds with calcium, yielding hypocalcemia. Lastly, uric acid, the breakdown product of purine metabolism, is released extracellularly, resulting in hyperuricemia. These derangements can cause nephropathy due to uric acid or calcium phosphate precipitation in the kidney tubules, which, along with volume depletion, can result in acute kidney injury. Lastly, the Cairo-Bishop classification system can be utilized to make the final diagnosis of TLS, which is a either a laboratory diagnosis (two of four lab abnormalities), or a clinical diagnosis (one lab abnormality with a clinical presentation [seizure, acute kidney injury, arrhythmia, etc.]). The recommended workup for TLS is listed in Table 1.[2]
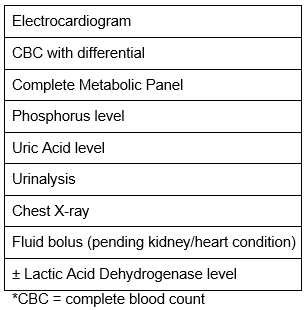 |
| Table 1: Tumor Lysis Syndrome Order Set |
Hyperuricemia and hyperphosphatemia are typically clinically silent, but comparatively, hyperkalemia and hypocalcemia can present with a myriad of symptoms. Like any other medical condition that results in hyperkalemia, TLS-related hyperkalemia is identical and can present with muscle cramps, fatigue, paresthesias, or cardiac arrhythmias. “CATS go numb,” on the other hand, is the mnemonic for hypocalcemia-related symptoms (convulsions, arrhythmias, tetany, spasms and stridor, and numbness in the fingers.
Risk factors for developing this syndrome include high tumor burden, rapidly progressing malignancy (leukemia, lymphoma, white blood count greater than 100,000), dehydration, chronic kidney disease, and associated nephrotoxins (which includes many chemotherapy agents). The key to treating TLS appropriately lies in making the diagnosis, which can easily be overlooked. The mainstay of treatment is hydration, attempting to achieve diuresis of 100-200 mL/hour. Depending on the electrolyte abnormality, such as hyperkalemia, one can initiate dialysis or utilize other methods to remove or shift potassium. Regarding uric acid, rasburicase is the first line treatment. Allopurinol can be used for prevention or if there is a contraindication to rasburicase, such as glucose-6-phosphate dehydrogenase deficiency.[2,3]
Regarding identifying this disease and subsequently managing it, the prognosis regarding mortality if it was sudden onset can range from 15-36%. This most likely warrants ICU admission pending the patient’s clinical appearance.[3]
References:
1. Brown J, Grudzen C, Kyriacou DN, et al. The emergency care of patients with cancer: setting the research agenda. Ann Emerg Med. 2016;68(6): 706-11.
2. Howard S, Jones D, Ching-Hon P. Tumor lysis syndrome. N Engl J Med. 2011;364(19):1844-54.
3. Gupta A, Moore J. Tumor lysis syndrome. JAMA Oncol. 2018;4(6):895