

Author: Meaghan Mercer, DO
Emergency Medicine Resident
University of Nevada School of Medicine
AAEM/RSA Immediate Past President
 |
| This post was peer reviewed. Click to learn more. |
The following blog post appeared initially at www.lasvegasemr.com/foam-blog and is reproduced with the permission of the author.
Case:
A 40-year-old female presents to the emergency department with a chief complaint of three days of palpitations. An EKG is performed and is shown below. Her past medical history includes hypertension and paroxysmal atrial fibrillation, but she has never had a thrombotic event. She was taking warfarin 5mg/day but ran out of her medications two days ago. You perform a bedside cardiac ultrasound and do not see any large thrombus. Complete blood count, basic metabolic panel, and troponin are all normal and her international normalized ratio (INR) is 1.5.
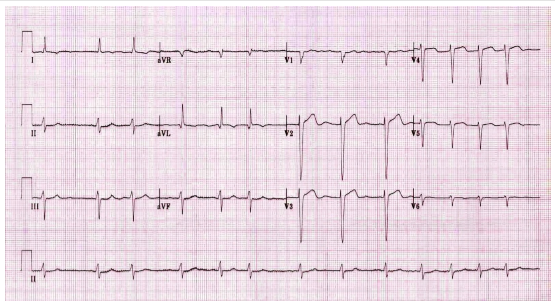
EKG found for free here: http://lifeinthefastlane.com/ecg-library/atrial-fibrillation/
What is the next step in her management?
A. Give the patient 5mg of warfarin in the ED and a prescription and discharge the patient home.
B. Put the patient on a bridging agent until INR is therapeutic.
C. Cardiovert the patient and send her home.
D. Switch the patient from warfarin to a different agent.
Answer: A
Background:
Warfarin (Coumadin) is an anticoagulant used to prevent thrombosis. Recall that Virchow’s triad describes the three factors that contribute to clot formation: blood stasis, hypercoagulability and endothelial dysfunction. Anticoagulation may be necessary in conditions that lead to stasis (immobilization, venous obstruction, atrial fibrillation), hypercoagulability (pregnancy, malignancy, protein C & S deficiency), and endothelial dysfunction (vascular injury, abnormal valves). Warfarin has a narrow therapeutic range and patients can become subtherapeutic for numerous reasons including: missed dose, dietary modifications, drug interactions, or dose reductions.
For warfarin to have an antithrombotic effect, prothrombin (Factor II) must decrease, and prothrombin’s half-life can be as long as three days. To protect against thrombotic events patients are often placed on bridging therapy with heparin. Once the INR reaches goal, bridging therapy is discontinued. Patients on chronic warfarin therapy have their INR monitored to ensure that it is within the therapeutic range.
Subtherapeutic INRs are associated with an increased risk of thrombosis. Patients who present to the ED with subtherapeutic values need to be assessed to see if bridging therapy is indicated. In a systematic review and metaregression of 67 studies that included 50,208 patients, 36.4% were found to have an INR out of the therapeutic range.[1] One study looking at the lowest effective intensity of prophylactic anticoagulation in atrial fibrillation found that patients with an INR of 1.7 had nearly twice the risk of stroke when compared to patients with an INR of 2.0. Similarly, an INR of 1.3 conferred a seven-fold risk.[2]
There is little data on whether bridging therapy with heparin is necessary in patients with a subtherapeutic INR. Most of the studies are retrospective analyses of patients who had their warfarin discontinued for an invasive procedure.
A retrospective study by Clark, et al., [3] looked at 2,597 patients on warfarin therapy and demonstrated the significance of a subtherapeutic INR. Patients with a single INR ≤0.5 lower than their target goal were placed in “low INR” cohort. The study’s primary outcome was any anticoagulation-related thromboembolic event measured at 90 days. Forty-six percent of patients were on warfarin for atrial fibrillation. The study found that 0.4% of patients in the low INR cohort had a thromboembolic event while 0.1% of patients in the therapeutic INR cohort had a thromboembolic event. The authors concluded that patients on stable warfarin therapy who experience a significant subtherapeutic INR value are at low risk for thromboembolism.
The American College of Chest Physicians published guidelines in the journal Chest regarding the approach to patients with subtherapeutic INR.[4]
- For patients with stable therapeutic INRs presenting with a single subtherapeutic INR value, administering bridging with heparin is not recommended. (Grade 2C).
- For patients taking vitamin K antagonists with previously stable therapeutic INRs who present with a single out-of-range INR of ≤0.5 below or above therapeutic, it is appropriate to continue the current dose and testing the INR within 1 to 2 weeks (Grade 2C).
Note that both recommendations apply only for a single subtherapeutic INR, not for multiple low INR values or patients who are off their medication. In addition, these guidelines do not directly address if bridging therapy should be initiated if a patient has >0.5 reduction in INR when compared to baseline goals.
One method that has been discussed to address subtherapeutic INRs greater than 0.5 away from the therapeutic range involves risk stratification of the patient using their CHADS2 score and other factors. If the patient is high risk, bridging therapy should be strongly considered.[3] If the patient has a medium risk, no strong guidelines exist to guide therapy, but studies suggest patients may not need bridging therapy. Future studies need to be done and strong guidelines need to be provided to direct management.
Managing our patient:
What is her CHADS2 score?
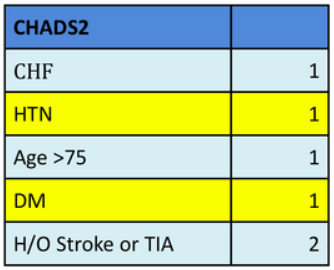
Answer: Two
What treatment is appropriate?
She has a single subtherapeutic INR and is at low risk for a thromboembolism. Per the guidelines provided by the American College of Chest Physicians [4], she can be given her usual dose and should have her INR rechecked in 1-2 weeks.
References
- Van Walraven C, Jennings A, Oake N, Fergusson D, Forster AJ. Effect of study setting on anticoagulation control: a systematic review and metaregression. Chest. 2006;129(5):1155-66. http://www.ncbi.nlm.nih.gov/pubmed/16685005
- Hylek EM, Skates SJ, Sheehan MA, Singer DE. An analysis of the lowest effective intensity of prophylactic anticoagulation for patients with nonrheumatic atrial fibrillation. N Engl J Med. 1996;335(8):540-6.
- Clark NP, Witt DM, Delate T, et al. Thromboembolic consequences of subtherapeutic anticoagulation in patients stabilized on warfarin therapy: the low INR study. Pharmacotherapy. 2008; 28(8):960-7.
- Holbrook A, Schulman S, Witt DM, et al. Evidence-based management of anticoagulant therapy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141(2 Suppl):e152S-84S.